Prescription Drug Program Manual
Printing the manual material found at this website for long-term use is not advisable. Department Policy material is updated periodically and it is the responsibility of the users to check and make sure that the policy they are researching or applying has the correct effective date for their circumstances.
If you experience any difficulty opening a section or link from this page, please email the webmaster.
How to Search this manual:
This edition has three search options.
- Search the whole manual. Open the Complete Manual tab. From your keyboard press the Ctrl and F keys at the same time. A search box will appear. Type in a descriptive or key word (for example "Denials"). The search box will show all locations where denials are discussed in the manual.
- Search by Chapter. Open any Chapter tab (for example the "Billing Procedures" tab). From your keyboard press the Ctrl and F keys at the same time. A search box will appear. Type in a descriptive or key word (for example "Denials"). The search box will show where denials are discussed in just that chapter.
- Site Search. Search the manual as well as other documents related to a particular search term on the Montana Healthcare Programs Site Specific Search page.
Prior manuals may be located through the provider website archives.
Updated 07/24/2025
Prescription Drug Program Manual
To print this manual, right click your mouse and choose "print". Printing the manual material found at this website for long-term use is not advisable. Department Policy material is updated periodically, and it is the responsibility of the users to check that the policy they are researching or applying has the correct effective date for their circumstances.
Update Log
Publication History
This publication supersedes all previous Prescription Drug Program Manuals. Published by the Montana Department of Public Health & Human Services, July 2001.
Updated October 2001, December 2001, May 2002, June 2002, September 2002, January 2003, August 2003, July 2004, November 2004, May 2011, August 2011, October 2011, December 2011, January 2013, March 2013, July 2013, September 2013, March 2015, June 2015, January 2016, July 2016, October 2016, December 2016, August 2017, February 2018, July 2018, November 2018, July 2019, January 2020, July 2020, April 2021, October 2021, July 2022, July 2023, April 2024, February 2025 and July 2025.
CPT codes, descriptions and other data only are copyright 2014 American Medical Association (or such other date of publication of CPT). All Rights reserved. Applicable FARS/DFARS Apply.
Update Log
07/24/2025
- Dispensing Fee updates
- Vaccine Administration Fee updates
- Updated Prior Authorization chapter
02/04/2025
- Dispensing Fee updates
- Vaccine Administration Fee updates
04/26/2024
- Dispensing Fee updates
07/05/2023
- Revised Covered Products chapter
07/21/2022
- Updated Key Contacts, Dispensing Limitations, Prior Authorization, Reimbursement, and Billing Procedures chapters.
- Updated Index to Search Options
10/26/2021
Updated Montana Healthcare Programs Covered Products and Reimbursement chapters.
04/13/2021
Added the COVID-19 vaccine administration rates to the Reimbursement chapter.
07/01/2020
Updated dispensing fees and the vaccine administration fee.
01/01/2020
- Cost Share references removed, and Cost Share section changed to Co-Payments section.
- Term "Medicaid" replaced with "Montana Healthcare Programs" throughout the manual.
- Terms "client", "recipient" and "patient" replaced with "member".
07/08/2019
References to the MA-5 were replaced with references to the Universal Claim Form Version 1.2-02/2013 throughout the manual. Instructions for the Universal Claim Form replaced instructions for the MA-5 form. Seasonale® removed from the 34-day supply exception list. Vasopressors-midodrine removed from the drug classes considered for maintenance medications list.
11/27/2018
Reimbursement Chapter was updated with current rates.
07/31/2018
How to Bill Pharmacy Claims was added to the Billing Procedures chapter and obsolete language was removed from the Drug Program chapter.
07/10/2018
Dispensing Limitations was updated.
02/9/2018
Reimbursement rates were updated in the Reimbursement chapter.
09/26/2017
A portion of the Federal Maximum Allowable Cost section in the Reimbursement chapter was eliminated.
08/08/2017
Mental Health Services - Adult Manual converted to an HTML format and adapted to 508 Accessibility Standards.
06/15/2016
Prescription Drug Program, July 2016: Cost Share Updates
12/31/2015
Prescription Drug Program, January 2016: HELP Plan-Related Updates and Others
07/21/2015
Prescription Drug Program, Prior Authorization, Reimbursement, and Billing Procedures
03/25/2015
Prescription Drug Program, Entire Manual
09/27/2013
Prescription Drug Program, Reimbursement
09/05/2013
Prescription Drug Program, Entire Manual Including the New Passport Chapter. This set of replacement pages contains a terminology change ("client" to "member"); however, only content changes are marked with a change bar (black line).
04/17/2013
Prescription Drug Program, Key Contacts and Reimbursement
02/04/2013
Prescription Drug Program, Medicaid Covered Products
02/01/2012
Prescription Drug Program, Multiple Chapters
09/01/2011
Prescription Drug Program, Medicaid Covered Services and Reimbursement (Dispensing Fee) and MHSP Covered Products (Formulary Drugs)
06/17/2011
Prescription Drug Program; Entire manual has changed from last posted version.
11/16/2004
Prescription Drug Program, Updated Prescription Drug Prior Authorization Criteria
06/16/2004
Prescription Drug Program, Prior Authorization and HIPAA Updates
06/10/2004
Prior Authorization Additions
End of Update Log Chapter
Table of Contents
Key Contacts
Drug Program
Montana Healthcare Programs Covered Products
Dispensing Limitations
Prior Authorization
Prior Authorization for Retroactively Eligible Members
Reimbursement
Billing Procedures
Third Party Payer – Negative Payment Amounts
Psychiatric Residential Treatment Facility (PRTF) Non-Psychotropic Medications
Point-of-Sale
Billing a Paper Claim
Appendix A: Forms
Appendix B: Definitions and Acronyms
Appendix C: Search Options
End of Table of Contents Chapter
Key Contacts
Drug Prior Authorization
For all questions regarding drug prior authorization:
(800) 395-7961
(406) 443-6002 (Helena)
8 a.m. to 5 p.m., Monday–Friday
Mountain Time
Mail or fax backup documentation to:
Mountain Pacific
P.O. Box 5119
Helena, MT 59604
(800) 294-1350 Fax
(406) 513-1928 Fax Helena
Point-of-Sale (POS) Help Desk
For assistance with online POS claims adjudication:
Conduent, Atlanta
Technical POS Help Desk
(800) 365-4944
6 a.m. to midnight, Monday–Saturday;
10 a.m. to 9 p.m., Sunday
Eastern Time
Program Policy
For program policy questions:
(406) 444-2738 Phone
(406) 444-1861 Fax
Allied Health Services Bureau
1400 Broadway
P.O. Box 202951
Helena, MT 59620
End of Key Contacts Chapter
Drug Program
Thank you for your willingness to serve members of the Montana Healthcare Programs administered by the Department of Public Health and Human Services.
Manual Organization
This manual provides information specifically for Prescription Drug Program providers. Other essential information for providers is contained in the separate General Information for Providers Manual . Providers are responsible for reviewing both manuals.
Manual Maintenance
Notification of manual updates are provided through the weekly web postings under “Recent Website Posts” on the Home page of the Provider Information website. Older versions of the manual may be found through the Archive page on the Provider Information website. Printing the manual material found at this website for long-term use is not advisable. Department Policy material is updated periodically, and it is the responsibility of the users to make sure that the policy they are researching or applying has the correct effective date for their circumstances.
Rule References
Providers must be familiar with all current rules and regulations governing the Montana Healthcare Programs. Provider manuals are to assist providers in billing Montana Healthcare Programs; they do not contain all Montana Healthcare Programs rules and regulations. Rule citations in the text are a reference tool; they are not a summary of the entire rule. If a manual conflicts with a rule, the rule prevails. Links to rules are available on the Provider Information website. Paper copies of rules are available through the Secretary of State’s office. Choose the Contact Us option under the ARM menu. In addition to the general Montana Healthcare Programs rules outlined in the General Information for Providers Manual, the following rules and regulations are also applicable to the Prescription Drug Program:
- Code of Federal Regulations (CFR)
- 42 USC 1396r-8, Payment for Covered Outpatient Drugs
- Montana Codes Annotated (MCA)
- MCA 37-7-101 – MCA 37-7-1408, Pharmacy
- Administrative Rules of Montana (ARM)
- ARM 37.86.1101 – ARM 37.86.1105, Outpatient Drug Services
Claims Review (MCA 53-6-111, ARM 37.85.406)
The Department is committed to paying Montana Healthcare Programs providers’ claims as quickly as possible. Montana Healthcare Programs claims are electronically processed and usually are not reviewed by medical experts prior to payment to determine if the services provided were appropriately billed. Although the computerized system can detect and deny some erroneous claims, there are many erroneous claims which it cannot detect. For this reason, payment of a claim does not mean that the service was correctly billed, or the payment made to the provider was correct. Periodic retrospective reviews are performed which may lead to the discovery of incorrect billing or incorrect payment. If a claim is paid and the Department later discovers that the service was incorrectly billed or paid or the claim was erroneous in some other way, the Department is required by federal regulation to recover any overpayment, regardless of whether the incorrect payment was the result of Department or provider error or other cause.
Getting Questions Answered
The provider manuals are designed to answer most questions; however, questions may arise that require a call to a specific group (such as a program officer, Provider Relations, or a prior authorization unit). The Key Contacts chapter and the Contact Us link on the Provider Information website have important phone numbers and addresses. Montana Healthcare Programs manuals, provider notices, fee schedules, forms, and more are available on the Provider Information website.
Drug Program Goal
The Prescription Drug Program covers pharmaceuticals and pharmacist services to members served by the Department in the Montana Healthcare Programs.
Who May Prescribe, Administer, or Dispense Legend Drugs and Controlled Substances?
Primary authority for the prescribing of legend drugs and controlled substances comes from individual professional practice acts, usually in the section of the act which defines the scope of practice for the profession. The definition of scope of practice is the responsibility of the board that licenses the professional. Only those providers not excluded by federal programs are eligible.
DUR Board
The Drug Use Review (DUR) Board performs drug utilization review and educational interventions. Five pharmacists and four physicians comprise the DUR Board which is coordinated by a full-time registered Montana pharmacist. The DUR Board meets monthly to review utilization and advise the Department.
Drug Use Review (DUR) Board meetings are posted on the Provider website. On the Pharmacy page, click on the Drug Use Review (DUR) Board pane.
The DUR Board and The University of Montana Skaggs School of Pharmacy also advise the Department on its outpatient drug formulary. Drugs are evaluated for safety, effectiveness, and clinical outcome. Drugs recommended for formulary exclusion have no significant, clinically meaningful therapeutic advantage over drugs recommended for inclusion.
End of Drug Program Chapter
Montana Healthcare Programs Covered Products
What Drugs and Pharmaceutical Supplies Are Covered?
Drug coverage is limited to those products where the pharmaceutical manufacturer has signed a rebate agreement with the federal government. Federal regulations further allow states to impose restrictions on payment of prescription drugs through prior authorization and preferred drug lists (PDL).
The Montana Healthcare Programs Prescription Drug Program covers the following:
- Legend drugs, subject to the PDL and prior authorization requirements.
- Selective non-prescription (over the counter (OTC)) medications. See the OTC Coverage tab on the Pharmacy page of the website. Nursing facilities are responsible for providing OTC antacids, aspirin, and laxatives to their residents.
- Compounded prescriptions
- Contraceptive supplies and devices
- Federal law allows states the discretion to cover certain medications listed in 42 USC 1396r-8. Montana Healthcare Programs has opted to cover the following medications for all members, including Medicare Part D members:
- Prescription cough and cold medications
- Selective non-prescription (over the counter (OTC)) medications. See the OTC Coverage tab on the Pharmacy page of the website. Montana Healthcare Programs does not cover proton pump inhibitors or non-sedating antihistamines for Part D members when the member’s prescription drug plan covers these classes of drugs.
- Vitamins and minerals may be granted prior authorization when indicated for the treatment of an appropriate diagnosis.
What Drugs and Pharmaceutical Supplies Are Not Covered?
The Montana Healthcare Programs Prescription Drug Program does not reimburse for the following items or services:
- Drugs supplied by drug manufacturers who have not entered into a federal drug rebate agreement.
- Drugs supplied by other public agencies such as the United States Veterans Administration, United States Department of Health and Human Services, local health departments, etc.
- Drugs for Medicare Part D dual eligible members, except for drugs covered in #5 in the What Drugs and Pharmaceutical Supplies Are Covered? section above.
- Drugs prescribed:
- To promote fertility
- For erectile dysfunction
- For weight reduction
- For cosmetic purposes or hair growth
- For an indication that is not medically accepted as determined by the Department in consultation with federal guidelines, the DUR Board, or the Department medical and pharmacy consultants.
- Drugs designated as less-than-effective (DESI drugs) or drugs that are identical, similar, or related to such drugs.
- Drugs that are experimental, investigational, or of unproven efficacy or safety.
- Free pharmaceutical samples.
- Obsolete National Drug Code (NDC).
- Terminated drug products.
- Any drug, biological product, or insulin provided as part of, or incident to and in the same setting as, any of the following:
- Inpatient hospital setting
- Hospice services
- Outpatient hospital services emergency room visit
- Other laboratory and x-ray services
- Renal dialysis
- Incarceration
- Any of the following drugs:
- Outpatient nonprescription drugs (except those OTC products previously listed)
- Covered outpatient drugs for which the manufacturer seeks to require as a condition of sale that associated tests or monitoring services be purchased exclusively from the manufacturer or its designee.
- Medical supplies (non-drug items) are not covered under the Prescription Drug Program.
a. Exception: Contraceptive supplies and devices
The Montana Preferred Drug List
To address the rising costs of prescription drugs, Montana Healthcare Programs implemented a preferred drug list (PDL) in 2005. The Department of Public Health and Human Services uses this program to provide clinically effective and safe drugs to its members at the best available price.
The PDL addresses certain classes of medications and provides a selection of therapeutically effective products for which the Montana Healthcare Programs will allow payment without restriction in those targeted classes. The Department, through its Formulary Committee, designates this listing of preferred drugs as “preferred” based primarily on clinical efficacy. In the designated classes, drug products that are non-preferred on the PDL will require prior authorization.
The Department updates the PDL annually and periodically as new drugs and information become available.
The current Montana PDL can be found on the Preferred Drug Information tab on the Pharmacy Page of the Provider Information website. Providers may address questions regarding the PDL and requests for prior authorization to the Drug Prior Authorization Unit. (See the Key Contacts chapter) The PDL/Prior Authorization Help Line is for providers only. Montana Healthcare Programs members with questions can ask their providers or call the Member Help Line, (800) 362-8312.
Medicare Part B and Part D Drug Claims
Part D
Medicare added prescription drug coverage for its beneficiaries under the Medicare Modernization Act, 42 USC 1302 Sec. 1395. Members enrolled in Medicare Part A and/or Part B are eligible for Medicare Part D and are required to receive their drug benefits through a Medicare Prescription Drug Plan (PDP). Members enrolled in both Montana Healthcare Programs and Medicare are considered “dual eligible” and are auto-enrolled in a Medicare PDP if they do not choose a plan. The Montana Healthcare Programs reimbursement for outpatient drugs provided to a full-benefit dual eligible member will be limited to the excluded drugs identified in this chapter and the Part B drugs described in the following paragraph.
Part B
Claims cross over automatically if the provider’s NPI/API is on file with Montana Healthcare Programs. The taxonomy code for the pharmacy is required on the claim.
To bill paper claims:
- Submit your claims on a CMS-1500 form.
- Attach the Medicare EOMB.
- Use your NPI/API.
- Mail to the Claims Processing Unit, P.O. Box 8000, Helena, MT 59604.
- Providers using paper claims must wait 45 days after Medicare paid date to submit claims.
Part B Crossover Claims
Part B crossover claims will be reimbursed using the following “lower of” pricing methodology:
- Montana Healthcare Programs allowed minus the Medicare paid; or
- Medicare coinsurance plus Medicare deductible.
Montana Healthcare Programs allowed for the pharmacy supplying and dispensing fee is $4.94.
For an updated list of covered Part B drugs, visit the CMS website, https://www.cms.gov.
End of Montana Healthcare Programs Covered Products Chapter
Dispensing Limitations
Prescription Quantity (ARM 37.86.1102)
Medications may not be dispensed in quantities greater than a 34-day supply except where manufacturer packing cannot be reduced to a smaller quantity.
1. The following drug classes, with examples, are considered maintenance medications and may be dispensed up to a 90-day supply.
Drug Classes Considered for Maintenance Medications
Cardiovascular (Heart Health)
- Antiarrhythmics — digoxin, amiodarone
- Antihypertensives (Blood Pressure)
- Angiotensin Modulators and Combinations — benazepril, lisinopril, irbesartan, losartan, valsartan, losartan/HCTZ, valsartan/HCTZ, lisinopril/HCTZ, enalapril/HCTZ
- Calcium Channel Blockers and Combinations — amlodipine, nifedipine, verapamil, diltiazem, amlodipine/valsartan, amlodipine/benazepril, Exforge HCT
- Beta Blockers and Alpha Blockers — atenolol, propranolol, metoprolol, prazosin, doxazosin, terazosin, carvedilol
- Alpha Agonists — clonidine, guanfacine, methyldopa
- Vasodilators — hydralazine, minoxidil, isosorbide
- Diuretics — furosemide, bumetanide, torsemide, HCTZ, metolazone, chlorothiazide, indapamide, spironolactone, amiloride, triamterene/HCTZ, spironolactone/HCTZ, amiloride/HCTZ
- Antihyperlipidemics (Cholesterol) — atorvastatin, lovastatin, pravastatin, rosuvastatin, simvastatin, gemfibrozil, fenofibrate, ezetimibe
- Platelet Aggregation inhibitors and hemorrhelogic agents (Blood Thinners) — Aggrenox, aspirin, clopidogrel, dipyridamole, Effient, Brillinta, pentoxifylline
Diabetes
- Antihyperglycemic — glimepiride, glipizide, glyburide, metformin, acarbose, Glyset, glyburide/metformin
Central Nervous System
- Anticonvulsants (exclusions apply) — divalproex, ethosuximide, phenytoin, lamotrigine, levetiracetam, topiramate, zonisamide, carbamazepine, oxcarbazepine
- Anti-Parkinson's and Other Movement Disorders — carbidopa, amantadine, pramipexole, ropinirole, carbidopa-levodopa
- Skeletal Muscle Relaxants — baclofen, chlorzoxazone, cyclobenzaprine, methocarbamol, orphenadrine, tizanidine
Gastrointestinal
- Antacids — Tums, Maalox
- Anti-Ulcer — sucralfate, misoprostol
- H2-Inhibitors — famotidine, ranitidine
- Bile Salts — ursodiol
Renal System
- Incontinence — oxybutynin, Toviaz
- Electrolyte Depleters/Replacers — calcium acetate, Renagel, potassium chloride, Phos-Nak, potassium citrate
- Hyperuricemia (Gout) — allopurinol, probenecid
Respiratory
- Antihistamines — cetirizine, loratadine, levocetirizine
- Leukotriene Receptor Antagonist (Asthma/Allergies) — montelukast
- Other — theophylline
Men and Women’s Health
- Contraceptives (oral, transdermal, intravaginal)
- Prostate — alfuzosin, tamsulosin, finasteride, dutasteride
- Breast Cancer — tamoxifen
- Vitamin Supplementation (restrictions apply) — prenatal vitamins, vitamin B, vitamin D, folic acid
Other Body Systems
- Bone Strength — alendronate, raloxifene
- Thyroid/Antithyroid — levothyroxine, methimazole, propylthiouracil
- NSAIDs (Pain/Inflammation) — diclofenac, ibuprofen, indomethacin, meloxicam, naproxen, sulindac, celecoxib
2. No more than two prescriptions of the same drug may be dispensed in a calendar month except for the following:
- Antibiotics
- Schedule II through V drugs
- Antineoplastic agents
- Compounded prescriptions
- Prescriptions for suicidal members or members at risk for drug abuse
- Topical preparations
The DUR Board has set monthly limits on certain drugs. Use over these amounts requires prior authorization.
Prescription Refills
Prescriptions for non-controlled substances may be refilled after 75% of the estimated therapy days have elapsed. Prescriptions for controlled substances (CII-CV), Ultram (tramadol), Ultracet (tramadol/acetaminophen), carisoprodol, and gabapentin may be refilled after 90% of the estimated therapy days have elapsed. The POS system will deny a claim for “refill to soon” based on prescriptions dispensed on month-to-month usage.
A prescription may be refilled early only if the prescriber changes the dosage, or if the member was admitted to a nursing facility. The pharmacist must document any dosage change. In any circumstance, the provider must contact the Drug Prior Authorization Unit to receive approval. (See Key Contacts.)
Pharmacists who identify members who experience difficulties in managing their drug therapy may consider unit dose prescriptions (see below).
Generic Drugs
The Department has a mandatory generic edit in the claims processing system. The edit is enabled once there are two rebateable AB-rated generic drugs available in the marketplace. Typically, the first generic labeler will have a six-month period of market exclusivity. To maximize value to the State, the Department recommends dispensing the brand name drug over the generic during this period of market exclusivity. Brands may be preferred over generics in other instances where there is a net cost benefit to the Department. Brand over generic preferences are listed on the PDL. When there are “preferred brands” on the Department’s PDL, generic equivalent drugs will require a prior authorization.
For drugs not subject to PDL restrictions and for those drugs listed in the Dispense As Written (DAW) section of the Billing Procedures chapter, if the brand name drug is prescribed instead of a generic equivalent, the prescriber must get prior authorization.
Authorization is based on medical need such as adverse reactions or therapeutic failures (clinically demonstrated, observed and documented) which have occurred when the generic drug has been used.
Unit Dose Prescriptions
Pharmacy-packaged unit dose medications may be used to supply drugs to members in nursing facilities, group homes, and other institutional settings.
Members who are not in one of the above facilities may also be considered high-risk and eligible for unit dose packaging if they:
- Have one or more of the following representative disease conditions: Alzheimer’s disease, blood clotting disorders, cardiac arrhythmia, congestive heart failure, depression, bipolar, cancer, diabetes, epilepsy, HIV/AIDS, hypertension, schizophrenia, or tuberculosis; and
- Consume two or more prescribed concurrent chronic medications which are dosed at three or more intervals per day; or
- Have demonstrated a pattern of noncompliance that is potentially harmful to their health.
Unit dose prescriptions may not exceed the 34-day supply limit.
Compounding
The Department shall reimburse pharmacies for compounding drugs only if the member’s drug therapy needs cannot be met by commercially available dosage strengths and/or forms of the therapy.
Prescription claims for compound drugs shall be billed and reimbursed using the National Drug Code (NDC) number and quantity for each compensable ingredient in the compound. No more than 25 ingredients may be reimbursed in any compound. Reimbursement for each drug component shall be determined in accordance with ARM 37.86.1101. Prior authorization requirements for individual components of a compound must be met for reimbursement purposes. The Department does not consider reconstitution to be compounding.
The Department may reimburse for compounded non-rebateable API bulk powders and excipients on the Department’s drug formulary maintained in accordance with ARM 37.86.1102.
End of Dispensing Limitations Chapter
Prior Authorization
Prior Authorization for Covered Drugs
Many drug products require prior authorization before the pharmacist provides them to the member. Requests are reviewed for medical necessity.
- Grandfathering of medications does not apply if samples, patient assistance, or cash pay have been used to bypass criteria or Preferred Drug List (PDL) placement.
- To request prior authorization, providers must submit the necessary information to the Drug Prior Authorization Unit. See the Pharmacy Resources page on the Mountain Pacific website.
- The prescriber (e.g., physician) or pharmacy may submit requests by mail, telephone, or fax to:
Drug Prior Authorization Unit
Mountain Pacific
P.O. Box 5119
Helena, MT 59604
(406) 443-6002 or 800-395-7961 (Phone)
(406) 513-1928 or 800-294-1350 (Fax)
- Requests are reviewed and decisions made immediately in most cases. Decisions on requests with special circumstances that require further peer review are made within 24 hours. Requests received after the Drug Prior Authorization Unit’s regular working hours of 8 a.m. to 5 p.m., Monday through Friday, or on weekends or holidays, are considered received at the start of the next working day.
- An emergency 72-hour supply may be dispensed for emergency, after-hours, weekend, and holiday requests. Payment will be authorized by using a “3” in the Days Supply field and a value of “8” in the Prior Authorization Type Code field.
Prior Authorization for Retroactively Eligible Members
All prior authorization requirements must be met for retroactively eligible members.
When a member is determined retroactively eligible for Montana Healthcare Programs, the member should give the provider a Notice of Retroactive Eligibility (160-M).
The provider has 12 months from the date retroactive eligibility was determined to bill for those services.
Retroactive Montana Healthcare Programs eligibility does not allow a provider to bypass prior authorization requirements.
When a member becomes retroactively eligible for Montana Healthcare Programs, the provider may:
- Accept the member as a Montana Healthcare Programs member from the current date.
- Accept the member as a Montana Healthcare Programs member from the date retroactive eligibility was effective.
- Require the member to continue as a private-pay member.
Providers may choose whether to accept retroactive eligibility. (See the General Information for Providers Manual, Member Eligibility and Responsibilities chapter.) All prior authorization requirements must be met to receive Montana Healthcare Programs payment.
When submitting claims for retroactively eligible members, attach a copy of the Notice of Retroactive Eligibility (Form 160-M) to the claim if the date of service is more than 12 months earlier than the date the claim is submitted.
End of Prior Authorization Chapter
Reimbursement
Reimbursement for Covered Drugs
Reimbursement for covered brand and generic preferred drugs shall not exceed the lowest of:
- The provider’s usual and customary charge of the drug to the general public; or
- The allowed ingredient cost plus a professional dispensing fee. Where allowed ingredient cost is defined as the lower of:
- The Average Acquisition Cost (AAC); or
- Submitted ingredient cost.
- If an AAC rate is not available, drug reimbursement is determined at the lower of:
- Wholesale Acquisition Cost (WAC);
- Affordable Care Act Federal Upper Limit (ACA FUL); or
- Submitted ingredient cost.
Average Acquisition Cost
Average acquisition cost (AAC) is the calculated average drug ingredient cost per drug determined by direct pharmacy survey, wholesale survey, and other relevant cost information. The AAC rates are published online under the Pharmacy Provider webpage.
Submitted Ingredient Cost
Submitted Ingredient is a pharmacy’s actual ingredient cost. For drugs purchased under the 340B Drug Pricing Program, submitted ingredient cost means the actual 340B purchase price. For drugs purchased under the Federal Supply Schedule (FSS), submitted ingredient cost means the actual FSS purchase price.
Usual and Customary
The usual and customary charge is the price the provider most frequently charges the general public for the same drug. In determining “usual and customary” prices, the Department:
- Does not include prescriptions paid by third party payers, including health insurers, governmental entities, and Montana Healthcare Programs, in the general public.
- Includes discounts advertised or given (including but not limited to cash rebate, monetary price discount, coupon of value) to any segment of the general public.
- Uses the lower of the two pricing policies if a provider uses different pricing for “cash” and “charge” members.
- Will use the median price if during an audit, the most frequent price cannot be determined from pharmacy records.
Federal Maximum Allowable Cost (MAC)
- The Federal Upper Limit pricing set by the U.S. Department of Health and Human Services Centers for Medicare & Medicaid (CMS).
Dispensing Fee
- The dispensing fee assigned shall range between:
- The minimum of $4.11 and the maximum of $17.52 for pharmacies with an annual prescription volume between 0 and 39,999
- The minimum of $4.11 and the maximum of $15.17 for pharmacies with an annual prescription volume between 40,000 and 69,999; or
- The minimum is $4.11 and the maximum is $12.83 for pharmacies with an annual prescription volume greater than 70,000.
- The dispensing fee for each compounded drug shall be $12.50, $17.50, or $22.50 based on the level of effort required by the pharmacist.
- New pharmacy providers are assigned the maximum dispensing fee. Failure to comply with the six-month dispensing fee questionnaire requirement will result in assignment of a dispensing fee of the lowest calculated cost to dispense that year.
- Pharmacies may receive an additional $0.75 for dispensing pharmacy-packaged unit dose prescriptions.
- Dispensing fee surveys are available from the Department of Public Health and Human Services Prescription Drug Program. (See Key Contacts.)
Vaccine Administration Fee
Pharmacies can receive a vaccine administration fee. This fee is in lieu of the standard dispensing fee. The fee for the first vaccine administered will be $21.32; the fee for each additional vaccine administered will be $16.04.
For the COVID-19 vaccine, Montana Healthcare Programs will follow the Medicare established rates for the administration fee, which are different from the above rates.
The Remittance Advice
The remittance advice is the best tool providers have to determine the status of a claim. Remittance advices accompany payment for services rendered. The remittance advice provides details of all transactions that have occurred during the previous remittance advice cycle. Each line of the remittance advice represents all or part of a claim and explains whether the claim or service has been paid, denied, or suspended (also referred to as pending). If the claim was suspended or denied, the remittance advice also shows the reason. See the General Information for Providers Manual for more information on the remittance advice.
As of July 2013, all new providers were required to enroll in electronic funds transfer (EFT) and receive electronic remittance advices. Providers who enrolled prior to July 2013 who received paper checks or paper remittance advices were transitioned to the electronic-only system over time.
Credit Balances
Credit balances occur when claim adjustments reduce original payments causing the provider to owe money to the Department. These claims are considered in process and continue to appear on the remittance advice until the credit has been satisfied. Credit balances can be resolved in two ways:
- By working off the credit balance. Remaining credit balances can be deducted from future claims. These claims will continue to appear on consecutive remittance advices until the credit has been paid.
- By sending a check payable to DPHHS for the amount owed. This method is required for providers who no longer submit claims to Montana Healthcare Programs. Attach a note stating that the check is to pay off a credit balance and include your provider number. Send the check to Third Party Liability
Rebilling and Adjustments
Rebillings and adjustments are important steps in correcting any billing problems you may experience. Knowing when to use the rebilling process versus the adjustment process is important. When submitting a reversal (void) use a B2 NCPDP transaction and when submitting a rebilled claim or an adjustment use a B3 NCPDP transaction (void & rebill).
Timeframe for Rebilling or Adjusting a Claim
- Providers may resubmit or adjust any initial claim within the timely filing limits described in the Billing Procedures chapter of this manual. Depending on switch-vendor requirements, some point-of-sale adjustments must be completed within three months. In this case, adjustments may be submitted on paper within the timely filing limits.
- These time periods do not apply to overpayments that the provider must refund to the Department. After the 12-month time period, a provider may not refund overpayments to the Department by completing a claim adjustment. The provider may refund overpayments by issuing a check or asking the Third-Party Liability Unit to complete a gross adjustment.
Rebilling Montana Healthcare Programs
Rebilling is when a provider submits a claim or claim line to Montana Healthcare Programs that was previously submitted for payment but was either returned or denied. Pharmacy providers can rebill Montana Healthcare Programs via point-of-sale or on paper. Paper claims are often returned to providers before processing because information such as the NPI or authorized signature/date are missing or unreadable. See the Billing Procedures chapter for tips on preventing returned or denied claims.
When to Rebill Montana Healthcare Programs
- Claim Denied. Providers can rebill Montana Healthcare Programs when a claim is denied in full, as long as the claim was denied for reasons that can be corrected. When the entire claim is denied, check the Explanation of Benefits (EOB) code, make the appropriate corrections, and resubmit the claim (not an adjustment).
- Line Denied. When an individual line is denied on a multiple-line claim, correct any errors and rebill Montana Healthcare Programs. Either submit the denied service on a new Universal Claim Form Version 1.2-02/2013, or cross out paid lines and resubmit the form, or submit via point-of-sale. Do not use an adjustment form.
- Claim Returned. Rebill Montana Healthcare Programs when the claim is returned under separate cover. Occasionally, Montana Healthcare Programs is unable to process the claim and will return it to the provider with a letter stating that additional information is needed to process the claim. Correct the information as directed and resubmit your claim. Paper pharmacy claims should be billed on a Universal Claim Form Version 1.2-02/2013.
How to Rebill
- Check any EOB code listed and make your corrections on a copy of the claim, or produce a new claim with the correct information, or rebill using point-of-sale.
- When making corrections on a copy of the claim, remember to cross out or omit all lines that have already been paid. The claim must be neat and legible for processing.
- Enter any insurance (third party liability) information on the corrected claim, or attach insurance denial information to the corrected claim, and send it to Claims Processing.
Adjustments
If a provider believes that a claim has been paid incorrectly, the provider may call Provider Relations. Once an incorrect payment has been verified, the provider may submit an Individual Adjustment Request form to Provider Relations or submit an adjustment through point-of-sale. If incorrect payment was the result of a Conduent keying error, the provider should contact Provider Relations.
When adjustments are made to previously paid claims, the Department recovers the original payment and issues appropriate repayment. The result of the adjustment appears on the provider’s RA as two transactions. The original payment will appear as a credit transaction. The replacement claim reflecting the corrections will be listed as a separate transaction and may or may not appear on the same remittance advice as the credit transaction. The replacement transaction will have nearly the same ICN number as the credit transaction, except the 12th digit will be a 2, indicating an adjustment. Adjustments are processed in the same time frame as claims.
When to Request an Adjustment
- • Request an adjustment when a claim was overpaid or underpaid.
• Request an adjustment when a claim was paid but the information on the claim was incorrect (e.g., member ID, NPI, date of service, NDC, prescribing provider, units).
How to Request an Adjustment
To request an adjustment, use the Individual Adjustment Request form. Adjustments may also be made using point-of-sale. The requirements for adjusting a claim are as follows:
- Claims Processing must receive individual claim adjustment requests within 12 months of the date of service. (See Timely Filing Limits in the Billing Procedures chapter.) After this time, gross adjustments are required.
- Use a separate adjustment request form for each TCN.
- If you are correcting more than one error per TCN, use only one adjustment request form, and include each error on the form.
- If more than one line of the claim needs adjusting, indicate which lines and items need to be adjusted in the Remarks section of the adjustment form.
Completing an Adjustment Request Form
- You may download the Individual Adjustment Request form from the Provider Information website. Complete Section A first with provider and member information and the claim’s TCN.
- Complete Section B with information about the claim. Complete only the items that need to be corrected. (See the table on next page.)
- Enter the date of service or the line number in the Date of Service or Line Number column.
- Enter the information from the claim that was incorrect in the Information on Statement column.
- Enter the correct information in the Corrected Information column.
- Attach copies of the remittance advice and a corrected claim if necessary.
- If the original claim was billed electronically, a copy of the remittance advice will suffice.
- If the remittance advice is electronic, attach a screen print of it.
- Verify the adjustment request has been signed and dated.
- Send the adjustment request to Claims Processing.
- If an original payment was an underpayment by Montana Healthcare Programs, the adjustment will result in the provider receiving the additional payment amount allowed.
- If an original payment was an overpayment by Montana Healthcare Programs, the adjustment will result in recovery of the overpaid amount through a credit balance or a check from the provider. (See Credit Balances earlier in this chapter.)
- Any questions regarding claims or adjustments must be directed to Provider Relations.
Completing an Individual Adjustment Request Form
Section A
Field: 1. Provider Name and Address
Description: Provider’s name and address (and mailing address if different).
Field: 2. Member Name
Description: The member’s name.
Field: 3.* Internal Control Number (ICN)
Description: There can be only one TCN per Adjustment Request form. When adjusting a claim that has been previously adjusted, use the TCN of the most recent claim.
Field: 4*. Provider NPI/API
Description: The provider’s NPI/API
Field: 5*. Member's Montana Healthcare Programs Number
Description: Member's Montana Healthcare Programs ID number.
Field: 6. Date of Payment
Description: Date claim was paid found on Remittance Advice Field 5 (see the sample RA earlier in this chapter).
Field: 7. Amount of Payment
Description: The amount of payment from the Remittance Advice Field 19 (see the sample RA earlier in this chapter.).
Section B
Field: 1. Units of Service
Description: If a payment error was caused by an incorrect number of units, complete this line.
Field: 2. Procedure Code/NDC/Revenue Code
Description: If the procedure code, NDC, or revenue code are incorrect, complete this line.
Field: 3. Dates of Service (DOS)
Description: If the date of service is incorrect, complete this line.
Field: 4. Billed Amount
Description: If the billed amount is incorrect, complete this line.
Field: 5. Personal Resource (Nursing Facility)
Description: If the member's personal resource amount is incorrect, complete this line.
Field: 6. Insurance Credit Amount
Description: If the member’s insurance credit amount is incorrect, complete this line.
Field: 7. Net (Billed - TPL or Medicare Paid)
Description: If the payment error was caused by a missing or incorrect insurance credit, complete this line. Net is billed amount minus the amount TPL or Medicare paid.
Field: 8. Other/Remarks
Description: If none of the above items apply, or if you are unsure what caused the payment error, complete this line.
*Indicates a required field
Mass Adjustments
Mass adjustments are done when it is necessary to reprocess multiple claims. They generally occur when:
- Montana Healthcare Programs has a change of policy or fees that is retroactive. In this case federal laws require claims affected by the changes to be mass adjusted.
- A system error that affected claims processing is identified.
Providers are informed of mass adjustments by a provider notice or on the first page of the remittance advice. Mass adjustment claims shown on the RA have an ICN that begins with a 4.
Payment and the Remittance Advice
Providers receive their Montana Healthcare Programs payment and remittance advices weekly. To sign up for EFT (direct deposit) and register for the web portal to view or download remittance advices, providers need to complete the EFT and ERA Authorization Agreement and the EDI Trading Partner Agreement and mail or fax them to Provider Relations. See the Provider Enrollment page for those documents.
A letter from your financial institution verifying legitimacy of the account is also required. The letter must include the name and contact information of the bank representative and be signed by the bank representative. Do not send voided checks or deposit slips.
Once enrolled in EFT and registered for the MATH web portal, providers are able to receive their electronic remittance advices. Due to space limitations, each remittance advice is available on the web portal for 90 days.
For assistance on enrolling in EFT, completing the EDI Trading Partner Agreement, and registering for the MATH web portal, contact Provider Relations.
End of Reimbursement Chapter
Billing Procedures
How to Bill Pharmacy Claims
- The Department supports NCPDP X2 Version D.0 electronic transactions.
- If a claim must be billed on paper, the Department supports the Universal Claim Form Version 1.2 - 02/2013.
- Pharmacies are eligible to receive five free Universal Claim Forms per year through NCPDP. To obtain a copy, please call (480) 477-1000.
- If a pharmacy needs more paper forms, they can be ordered through CommuniForm LLC via phone (877) 817-3676 or fax at (866) 308-2036. Providers may also request online login access from CommuniForm LLC by calling (877) 817-3676 to order forms online.
- Pharmacies are eligible to receive five free Universal Claim Forms per year through NCPDP. To obtain a copy, please call (480) 477-1000.
Provider Number
- The Department uses the pharmacy’s NPI as the provider number for billing purposes.
- The Department-assigned provider number is used for payment and reporting purposes.
- Changes in pharmacy ownership or NABP (NCPDP) number must be reported immediately to ensure that payments are received by the billing owner. Contact Provider Relations to report all ownership changes.
Provider Enrollment
P.O. Box 4936
Helena, MT 59604
(800) 624-3958
(406) 442-1837
Tamper-Resistant Pads
Written prescriptions must contain all of the following.
- One or more industry-recognized features designed to prevent unauthorized copying of a completed or blank prescription form;
- One of more industry-recognized features designed to prevent the erasure or modification of information written on the prescription by the prescriber; and
- On or more industry-recognized features designed to prevent the use of counterfeit prescription forms.
Outpatient pharmacy claims for Montana Healthcare Programs require the prescription origin code to indicate the source of the prescription. Valid values for prescription origin code are:
- 0 – Not specified
- 1 – Written prescription
- 2 – Telephone
- 3 – Electronic
- 4 – Facsimile
How Long Do I Have to Bill?
Providers are required to submit a clean claim no later than 365 days from:
- The date of service;
- The date retroactive eligibility is determined;
- The date disability is determined; or
- Within 6 months of the date Medicare pays, whichever is later.
A clean claim is one that can be adjudicated without correction or additional information or documentation from the provider.
Prescription Tracking and Claim Reversals
For purposes of billing for prescribed drugs, the date of service means the date a prescription is filled. If the drug has not been received by the member or the member’s representative within 15 days after the prescription is filled, the pharmacy must reverse the claim and refund the payment to the Department.
Tips to Avoid Timely Billing Denials
- Correct and resubmit denied claims promptly. (See the Reimbursement chapter, Remittance Advices and Adjustments section in this manual.)
- If a claim submitted to Montana Healthcare Programs does not appear on the remittance advice within 30 days, contact Provider Relations for claim status.
When to Bill Montana Healthcare Programs Members (ARM 37.85.406)
In most circumstances, providers may not bill Montana Healthcare Programs members for services covered under Montana Healthcare Programs. More specifically, providers cannot bill members directly:
- For the difference between charges and the amount Montana Healthcare Programs paid.
- For a covered service provided to a Montana Healthcare Programs-enrolled member who was accepted as a Montana Healthcare Programs member by the provider, even if the claim was denied.
Under certain circumstances, providers may need a signed agreement in order to bill a Montana Healthcare Programs member (see the following table).
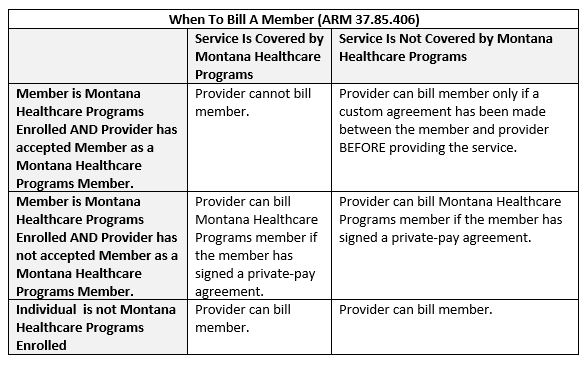
Routine Agreement: This may be a routine agreement between the provider and member which states that the member is not accepted as a Montana Healthcare Programs member, and that he/she must pay for the services received.
Custom Agreement: This agreement lists the service the member will receive and states that the service is not covered by Montana Healthcare Programs and that the member will pay for the services received.
Billing for Retroactively Eligible Members
When the provider accepts the member’s retroactive eligibility, the provider has 12-months from the date retroactive eligibility was determined to bill for those services.
When submitting claims for retroactively eligible members in which the date of service is more than 12 months earlier than the date the claim is submitted, attach a copy of the Provider Notice of Eligibility (Form 160-M). The provider must request the form from the member’s local Office of Public Assistance.
See the DPHHS Field Offices Public Assistance webpage. For more information on retroactive eligibility, see the Member Eligibility and Responsibilities chapter in the General Information for Providers Manual.
Usual and Customary Charge (ARM 37.85.406)
Providers should bill Montana Healthcare Programs their usual and customary charge for each service; that is, the same charge that is made to other payers for that service.
Member Co-Payment (ARM 37.85.204)
Effective for all claims paid on or after January 1, 2020 co-payment will not be assessed.
The provider must always use the complete 11-digit NDC from the dispensing container.
National Drug Codes (NDC)
All outpatient prescription drugs are billed using the drug’s NDC, the 11-digit code assigned to all prescription drug products by the labeler or distributor of the product under FDA regulations.
The Department accepts only the 5-4-2 NDC format. All 11 digits, including zeros, must be entered. The three segments of the NDC are:
SAMPLE NDC: 12345-6789-10
12345 = labeler code
6789 = product code
10 = package size
Claims must accurately report the NDC dispensed, the number of units dispensed, days supply, and the date of dispensing. Use of an incorrect NDC or inaccurate reporting of a drug quantity will cause the Department to report false data to drug manufacturers billed for drug rebates.
The Department will recover payments made on erroneous claims discovered during dispute resolution with drug manufacturers. Pharmacies are required to document purchase for quantities of brands of drugs reimbursed by the Department if disputes occur.
Dispense As Written (DAW)
Prescribers and pharmacies must prescribe and dispense the generic form of a drug whenever possible. Except for those drugs listed below, prior authorization is required when a brand name drug is prescribed instead of a generic equivalent. Please use the following DAW codes for these situations:
- DAW 1 may only be used if authorized by the Drug Prior Authorization Unit. In addition to prior authorization requirements, brand name drugs with a generic equivalent (except those required by the PDL) may be billed only when the prescriber has handwritten “brand necessary” or “brand required” on the prescription. The pharmacy must retain brand certifications as documentation.
- DAW 5 may be used in instances where the drug dispensed is generic but is listed as a brand (branded generics) and some cases a prior authorization is required.
- DAW 7 may be used for seizure medications with an appropriate diagnosis without prior authorization. Based on DUR Board recommendations only antiepileptic medications being used for a seizure diagnosis, and anti-hemophilic factors will continue to be considered narrow therapeutic index (NTI) drugs. A DAW 7 override will be allowed on these drugs only. See the 2009 provider notice on the Pharmacy page of the website for additional information.
- DAW 9 is used when a brand name multisource drug is preferred and pharmacy is dispensing the brand name drug, this exempts the pharmacy from using the generic and allows reimbursement at the brand name rate.
Abuse and Misutilization
The following practices constitute abuse and misutilization:
- Excessive Fees: Commonly known as prescription splitting or incorrect or excessive dispensing fees. Billing inappropriately in order to obtain dispensing fees in excess of those allowed by:
- Supplying medication in amounts less than necessary to cover the period of the prescription.
- Supplying multiple medications in strengths or quantities less than those prescribed to gain more than one dispensing fee.
- Excessive Filling: Billing for an amount of a drug or supply greater than the prescribed quantity.
- Prescription Shorting: Billing for drug or supply greater than the quantity actually dispensed.
- Substitution to Achieve a Higher Price: Billing for a higher priced drug than prescribed even though the prescribed lower priced drug was available.
Third Party Payer – Negative Payment Amounts
Montana Healthcare Programs will not approve a claim with a negative payment amount (from click fees or PBM clawbacks) or allow pharmacies to bypass the primary insurance to eliminate the negative payment amount. If a pharmacy receives a negative amount from the primary insurance and a member has Montana Healthcare Programs as secondary, the pharmacy must bill with the following to receive payment from the Department:
- Other Coverage Code = 4, defined as Other Coverage exists – payment not collected – NCPDP field (308-C8)
- Other Payer Amount – NCPDP field (431-DV) = $0.00
In addition, providers are reminded that aside from a member copayment, if there is one, payment from Montana Healthcare Programs is payment in full. Negative payment amounts may not be passed on to members.
Psychiatric Residential Treatment Facility (PRTF) Non-Psychotropic Medications
Pharmacies who fill medications for PRTFs are able to bill for non-psychotropic medications for members currently in an all-inclusive PRTF by submitting the claim with a submission clarification code (SCC) of 10 in NCPDP field (420-DK). If these pharmacies receive a claim rejection of “member enrolled in all-inclusive program, contact facility for payment” despite submitting with a SCC code of 10, this indicates the medication being billed is classified as a psychotropic medication and can’t be reimburse through the pharmacy benefit. Psychotropic medications are included in the all-inclusive payment and must be billed to the facility. However, if the medication is on the psychotropic list but is being used for a non-psychiatric diagnosis, a prior authorization may be obtained by calling the Drug Prior Authorization Unit at (406) 443-6002 or (800) 395-7961.
If pharmacies are trying to bill prescriptions for a member that has been released from an all-inclusive facility but are still getting denied claims with the same rejection referenced above, please contact the Pharmacy Program Officer or the Montana Healthcare Programs Pharmacist.
End of Billing Procedures Chapter
Point-of-Sale
What Is the Pharmacy Point-of-Sale (POS)?
The point-of-sale (POS) system finalizes claims at the point of entry as either paid or denied. Pharmacies arrange their own telecommunications switch services to accept Montana Healthcare Programs point of sale and are responsible for any charges imposed by these vendors. Hard copy (paper) billing is still accepted when billed on a Universal Claim Form Version 1.2-02/2013. All claims are processed and edited through the POS system regardless of how the claim was originally submitted.
If the claim continues to deny for eligibility past 3 working days, call Provider Relations at (800) 624-3958.
Possession of a Montana Access to Health (MATH) Montana Healthcare Programs ID card is not proof of eligibility.
Member eligibility may change monthly, so providers should verify eligibility each month. Both the 7-digit member number and the member’s Social Security number are billable numbers. If a claim is rejected online, a provider should verify eligibility by one of the methods (MATH web portal, IVR, FaxBack, calling Provider Relations) described in the General Information for Providers Manual.
Pro-DUR
The POS system performs all major prospective drug utilization review (Pro-DUR) edits. In some circumstances, the Pro-DUR edits result in denied claims. When a Pro-DUR denied claim needs to be overridden, pharmacy providers may enter one Reason for Service Code (formerly DUR Conflict Code) from each category in the following order, as long as the indicated situations exist and the pharmacy retains documentation in its files:
- Two-byte alpha Reason for Service Code, followed by...
- Two-byte alphanumeric Professional Service Code, followed by...
- Two-byte alphanumeric Result of Service Code
By placing codes into the claim, the provider is certifying that the indicated DUR code is true and documentation is on file. For questions regarding DUR codes, contact the Drug Prior Authorization Unit.
NCPDP DUR Codes
End of Point-of-Sale Chapter
Billing a Paper Claim
Completing a Universal Claim Form
Providers may also request online login access from CommuniForm LLC by calling (877) 817-3676. Forms can be ordered online by logging in on the Welcome page of the ACES Benefits website
Paper claims must be mailed to the following address:
Claims Processing Unit
P.O. Box 8000
Helena, MT 59604
Universal Claim Form Instructions
| Field Number | Field Title | Instructions |
|---|---|---|
| 1 | ID-Insurance | Enter the Member ID. |
| 2 | Group ID-Insurance | Enter the insurance Group ID. |
| 3 | Last-Insurance | Enter the last name of the member |
| 4 | First-Insurance | Enter the first name of the member. |
| 5 | Plan Name-Insurance | Enter the plan name for the member. |
| 6 | BIN #-Insurance | Enter the BIN number from the member ID Card. |
| 7 | Processor Control #-Insurance | Enter the PCN number from the member ID card. |
| 8 | CMS Part D Defined Qualified Facility | Enter a "Y" or "N" if the pharmacy is a CMS Part D Defined Qualified Facility. |
| 9 | Last-Member | Enter the member last name. |
| 10 | First-Member | Enter the member first name. |
| 11 | Person Code-Member | Enter the three digit person code. |
| 12 | D.O.B.-Member | Enter the member date of birth in MM-DD-CCYY format. |
| 13 | Gender-Member | Enter the member gender code. |
| 14 | Relationship-Member | Enter the relationship code between the member and cardholder. |
| 15 | Member Residence-member | Enter the member residence code. |
| 16 | DO NOT USE | Leave this field blank. |
| 17 | Service Provider ID-Pharmacy | Enter the pharmacy ID. |
| 18 | Qualifier-Pharmacy | Enter the service provider ID qualifier code. |
| 19 | Name-Pharmacy | Enter the name of the pharmacy. |
| 20 | Telephone #-Pharmacy | Enter the telephone number for the pharmacy. |
| 21 | Address-Pharmacy | Enter the address of the pharmacy. |
| 22 | City-Pharmacy | Enter the city of the pharmacy. |
| 23 | State-Pharmacy | Enter the State of the Pharmacy. |
| 24 | Zip-Pharmacy | Enter the zip code for the pharmacy. |
| 25 | Signature of Provider | The provider must sign this field. |
| 26 | Date | Enter the date in which the provider signed the paper claim. |
| 27 | ID-Prescriber | Enter the ID for the prescribing provider. |
| 28 | Qualifier-Prescriber | Enter the prescriber ID qualifier. |
| 29 | Last Name-Prescriber | Enter the prescriber's last name. |
| 30 | ID-Pharmacist | Enter the pharmacist's ID number. |
| 31 | Qualifier-Pharmacist | Enter the pharmacist's ID qualifier. |
| 32 | Prescription/Service Ref. #-Claim | Enter the Prescription or reference number. |
| 33 | Qual-Claim | Enter the prescription or service ID qualifier. |
| 34 | Fill #- Claim | Enter the fill number. |
| 35 | Date Written-Claim | Enter the date the prescription was written. |
| 36 | Date of Service-Claim | Enter the date of service. |
| 37 | Submission Clarification-Claim | Enter the submission clarification code. |
| 38 | Prescription Origin-Claim | Enter the prescription origin code. |
| 39 | Pharmacy Service Type-Claim | Enter the pharmacy service type code. |
| 40 | Special Packaging Indicator-Claim | Enter the special packaging indicator code. |
| 41 | Product/Service ID-Claim | Enter the product/service ID. |
| 42 | Qual-Claim | Enter the product/service ID qualifier. |
| 43 | Product Description-Claim | Enter the product description. |
| 44 | Quantity Dispensed-Claim | Enter the quantity dispensed. |
| 45 | Days Supply-Claim | Enter the days supply dispensed. |
| 46 | DAW Code- Claim | Enter the appropriate DAW code. |
| 47 | Prior Auth # Submitted-Claim | Enter the prior authorization number submitted. |
| 48 | PA Type-Claim | Enter the prior authorization type code. |
| 49 | Other Coverage-Claim | Enter the appropriate other coverage code, if applicable. |
| 50 | Delay Reason-Claim | Enter the appropriate delay reason code. |
| 51 | Level of Service-Claim | Enter the level of service. |
| 52 | Place of Service-Claim | Enter the place of service. |
| 53 | Quantity Prescribed-Claim | Enter the total quantity prescribed. |
| 54 | Diagnosis Code-Clinical | Enter the appropriate diagnosis code. |
| 55 | Qual-Clinical | Enter the diagnosis code qualifier. |
| 56 | DUR/PPS Codes- Reason-DUR | Enter the DUR/PPS reason for service code. |
| 57 | DUR/PPS Codes-Service-DUR | Enter the DUR/PPS service code. |
| 58 | DUR/PPS Codes-Result-DUR | Enter the DUR/PPS result of service code. |
| 59 | Level of Effort-DUR | Enter the level of effort-required when billing a compound. |
| 60 | Procedure Modifier-DUR | Enter the procedure modifier. |
| 61 | Other Payer ID-COB 1 | Enter the other payer ID when COB is present. |
| 62 | Qual-COB 1 | Enter the other payer ID qualifier. |
| 63 | Other Payer Date-COB 1 | Enter the date in which the other payer paid the claim. |
| 64 | Other Payer Rejects-COB 1 | Enter the other payer reject codes (maximum of 3). |
| 65 | Other Payer ID-COB 2 | Enter the other payer ID when COB is present. |
| 66 | Qual-COB 2 | Enter the other payer ID qualifier. |
| 67 | Other Payer Date-COB 2 | Enter the date in which the other payer paid the claim. |
| 68 | Other Payer Rejects-COB 2 | Enter the other payer reject codes (maximum of 3). |
| 69 | Dosage Form Description Code-Compound | Enter the dosage form description code. |
| 70 | Dispensing Unit Form Indicator-Compound | Enter the dispensing unit form indicator. |
| 71 | Route of Administration | Enter the SNOMED route of administration code. |
| 72 | Ingredient Component Count-Compound | Enter the ingredient component count code. |
| 73 | Product Name-Compound | Enter the product name (maximum of 25). |
| 74 | Product ID-Compound | Enter the product ID (maximum of 25). |
| 75 | Qual-Compound | Enter the product ID number qualifier (maximum of 25). |
| 76 | Ingredient QTY-Compound | Enter the ingredient quantity. |
| 77 | Ingredient Drug Cost-Compound | Enter the ingredient drug cost associated with the product ID. |
| 78 | Basis of Cost-Compound | Enter the basis of cost code. |
| 79 | Usual & Customary Charge-Pricing | Enter the usual and customary charge. |
| 80 | Basis of Cost Det.-Pricing | Enter the basis of cost determination. |
| 81 | Ingredient Cost Submitted Enter | Enter the submitted ingredient cost. |
| 82 | Dispensing Fee Submitted-Pricing | Enter the submitted dispensing fee. |
| 83 | Prof Service Fee Submitted-Pricing | Enter the submitted professional service fee. |
| 84 | Incentive Amount Submitted-Pricing | Enter the submitted incentive amount. |
| 85 | Other Amount Submitted-Pricing | Enter the submitted other amount. |
| 86 | Sales tax Submitted-Pricing | Enter the submitted sales tax. |
| 87 | Gross Amount Due (submitted)-Pricing | Enter the submitted gross amount due. |
| 88 | Member Paid Amount | Enter the amount paid by the member. |
| 89 | Other Payer Amount Paid #1-Pricing | Enter the other payer amount paid by the first other payer (if present). |
| 90 | Other Payer Amount Paid #2 | Enter the other payer amount paid by the second other payer (if present). |
| 91 | Other Payer Member Resp. Amount #1-Pricing | Enter the other payer member responsibility amount from the first other Payer (if present). |
| 92 | Payer Member Resp. Amount #2-Pricing | Enter the other payer member responsibility amount from the second other Payer (if present). |
| 93 | Net Amount Due-Pricing | Enter the net amount due. |
End of Billing a Paper Claim Chapter
Appendix A: Forms
The forms below and others are available on the Forms page of the Provider Information website:
- Drug Prior Authorization Form
- Individual Adjustment Request
- Link Request, Montana Access to Health Web Portal
- Prescription Claim Form UCF (Universal Claim Form Version 1.2-02/2013)
End of Appendix A: Forms Chapter
Definitions and Acronyms
End of Definitions and Acronyms Chapter
Search Options
This edition has three search options.
- Search the whole manual. Open the Complete Manual tab. From your keyboard press the Ctrl and F keys at the same time. A search box will appear. Type in a descriptive or key word (for example "Denials"). The search box will show all locations where denials are discussed in the manual.
- Search by Chapter. Open any Chapter tab (for example the "Billing Procedures" tab). From your keyboard press the Ctrl and F keys at the same time. A search box will appear. Type in a descriptive or key word (for example "Denials"). The search box will show where denials are discussed in just that chapter.
- Site Search. Search the manual as well as other documents related to a particular search term on the Site Specific Search page.
End of Search Options Chapter
End of Prescription Drug Program Manual
Prescription Drug Program Manual
To print this manual, right click your mouse and choose "print". Printing the manual material found at this website for long-term use is not advisable. Department Policy material is updated periodically, and it is the responsibility of the users to check that the policy they are researching or applying has the correct effective date for their circumstances.
Update Log
Publication History
This publication supersedes all previous Prescription Drug Program Manuals. Published by the Montana Department of Public Health & Human Services, July 2001.
Updated October 2001, December 2001, May 2002, June 2002, September 2002, January 2003, August 2003, July 2004, November 2004, May 2011, August 2011, October 2011, December 2011, January 2013, March 2013, July 2013, September 2013, March 2015, June 2015, January 2016, July 2016, October 2016, December 2016, August 2017, February 2018, July 2018, November 2018, July 2019, January 2020, July 2020, April 2021, October 2021, July 2022, July 2023, April 2024, February 2025 and July 2025.
CPT codes, descriptions and other data only are copyright 2014 American Medical Association (or such other date of publication of CPT). All Rights reserved. Applicable FARS/DFARS Apply.
Update Log
07/24/2025
- Dispensing Fee updates
- Vaccine Administration Fee updates
- Updated Prior Authorization chapter
02/04/2025
- Dispensing Fee updates
- Vaccine Administration Fee updates
04/26/2024
- Dispensing Fee updates
07/05/2023
- Revised Covered Products chapter
07/21/2022
- Updated Key Contacts, Dispensing Limitations, Prior Authorization, Reimbursement, and Billing Procedures chapters.
- Updated Index to Search Options
10/26/2021
Updated Montana Healthcare Programs Covered Products and Reimbursement chapters.
04/13/2021
Added the COVID-19 vaccine administration rates to the Reimbursement chapter.
07/01/2020
Updated dispensing fees and the vaccine administration fee.
01/01/2020
- Cost Share references removed, and Cost Share section changed to Co-Payments section.
- Term "Medicaid" replaced with "Montana Healthcare Programs" throughout the manual.
- Terms "client", "recipient" and "patient" replaced with "member".
07/08/2019
References to the MA-5 were replaced with references to the Universal Claim Form Version 1.2-02/2013 throughout the manual. Instructions for the Universal Claim Form replaced instructions for the MA-5 form. Seasonale® removed from the 34-day supply exception list. Vasopressors-midodrine removed from the drug classes considered for maintenance medications list.
11/27/2018
Reimbursement Chapter was updated with current rates.
07/31/2018
How to Bill Pharmacy Claims was added to the Billing Procedures chapter and obsolete language was removed from the Drug Program chapter.
07/10/2018
Dispensing Limitations was updated.
02/9/2018
Reimbursement rates were updated in the Reimbursement chapter.
09/26/2017
A portion of the Federal Maximum Allowable Cost section in the Reimbursement chapter was eliminated.
08/08/2017
Mental Health Services - Adult Manual converted to an HTML format and adapted to 508 Accessibility Standards.
06/15/2016
Prescription Drug Program, July 2016: Cost Share Updates
12/31/2015
Prescription Drug Program, January 2016: HELP Plan-Related Updates and Others
07/21/2015
Prescription Drug Program, Prior Authorization, Reimbursement, and Billing Procedures
03/25/2015
Prescription Drug Program, Entire Manual
09/27/2013
Prescription Drug Program, Reimbursement
09/05/2013
Prescription Drug Program, Entire Manual Including the New Passport Chapter. This set of replacement pages contains a terminology change ("client" to "member"); however, only content changes are marked with a change bar (black line).
04/17/2013
Prescription Drug Program, Key Contacts and Reimbursement
02/04/2013
Prescription Drug Program, Medicaid Covered Products
02/01/2012
Prescription Drug Program, Multiple Chapters
09/01/2011
Prescription Drug Program, Medicaid Covered Services and Reimbursement (Dispensing Fee) and MHSP Covered Products (Formulary Drugs)
06/17/2011
Prescription Drug Program; Entire manual has changed from last posted version.
11/16/2004
Prescription Drug Program, Updated Prescription Drug Prior Authorization Criteria
06/16/2004
Prescription Drug Program, Prior Authorization and HIPAA Updates
06/10/2004
Prior Authorization Additions
End of Update Log Chapter
Table of Contents
Key Contacts
Drug Program
Montana Healthcare Programs Covered Products
Dispensing Limitations
Prior Authorization
Prior Authorization for Retroactively Eligible Members
Reimbursement
Billing Procedures
Third Party Payer – Negative Payment Amounts
Psychiatric Residential Treatment Facility (PRTF) Non-Psychotropic Medications
Point-of-Sale
Billing a Paper Claim
Appendix A: Forms
Appendix B: Definitions and Acronyms
Appendix C: Search Options
End of Table of Contents Chapter
Key Contacts
Drug Prior Authorization
For all questions regarding drug prior authorization:
(800) 395-7961
(406) 443-6002 (Helena)
8 a.m. to 5 p.m., Monday–Friday
Mountain Time
Mail or fax backup documentation to:
Mountain Pacific
P.O. Box 5119
Helena, MT 59604
(800) 294-1350 Fax
(406) 513-1928 Fax Helena
Point-of-Sale (POS) Help Desk
For assistance with online POS claims adjudication:
Conduent, Atlanta
Technical POS Help Desk
(800) 365-4944
6 a.m. to midnight, Monday–Saturday;
10 a.m. to 9 p.m., Sunday
Eastern Time
Program Policy
For program policy questions:
(406) 444-2738 Phone
(406) 444-1861 Fax
Allied Health Services Bureau
1400 Broadway
P.O. Box 202951
Helena, MT 59620
End of Key Contacts Chapter
Drug Program
Thank you for your willingness to serve members of the Montana Healthcare Programs administered by the Department of Public Health and Human Services.
Manual Organization
This manual provides information specifically for Prescription Drug Program providers. Other essential information for providers is contained in the separate General Information for Providers Manual. Providers are responsible for reviewing both manuals.
Manual Maintenance
Notification of manual updates are provided through the weekly web postings under “Recent Website Posts” on the Home page of the Provider Information website. Older versions of the manual may be found through the Archive page on the Provider Information website. Printing the manual material found at this website for long-term use is not advisable. Department Policy material is updated periodically, and it is the responsibility of the users to make sure that the policy they are researching or applying has the correct effective date for their circumstances.
Rule References
Providers must be familiar with all current rules and regulations governing the Montana Healthcare Programs. Provider manuals are to assist providers in billing Montana Healthcare Programs; they do not contain all Montana Healthcare Programs rules and regulations. Rule citations in the text are a reference tool; they are not a summary of the entire rule. If a manual conflicts with a rule, the rule prevails. Links to rules are available on the Provider Information website. Paper copies of rules are available through the Secretary of State’s office. Choose the Contact Us option under the ARM menu. In addition to the general Montana Healthcare Programs rules outlined in the General Information for Providers Manual, the following rules and regulations are also applicable to the Prescription Drug Program:
- Code of Federal Regulations (CFR)
- 42 USC 1396r-8, Payment for Covered Outpatient Drugs
- Montana Codes Annotated (MCA)
- MCA 37-7-101 – MCA 37-7-1408, Pharmacy
- Administrative Rules of Montana (ARM)
- ARM 37.86.1101 – ARM 37.86.1105, Outpatient Drug Services
Claims Review (MCA 53-6-111, ARM 37.85.406)
The Department is committed to paying Montana Healthcare Programs providers’ claims as quickly as possible. Montana Healthcare Programs claims are electronically processed and usually are not reviewed by medical experts prior to payment to determine if the services provided were appropriately billed. Although the computerized system can detect and deny some erroneous claims, there are many erroneous claims which it cannot detect. For this reason, payment of a claim does not mean that the service was correctly billed, or the payment made to the provider was correct. Periodic retrospective reviews are performed which may lead to the discovery of incorrect billing or incorrect payment. If a claim is paid and the Department later discovers that the service was incorrectly billed or paid or the claim was erroneous in some other way, the Department is required by federal regulation to recover any overpayment, regardless of whether the incorrect payment was the result of Department or provider error or other cause.
Getting Questions Answered
The provider manuals are designed to answer most questions; however, questions may arise that require a call to a specific group (such as a program officer, Provider Relations, or a prior authorization unit). The Key Contacts chapter and the Contact Us link on the Provider Information website have important phone numbers and addresses. Montana Healthcare Programs manuals, provider notices, fee schedules, forms, and more are available on the Provider Information website.
Drug Program Goal
The Prescription Drug Program covers pharmaceuticals and pharmacist services to members served by the Department in the Montana Healthcare Programs.
Who May Prescribe, Administer, or Dispense Legend Drugs and Controlled Substances?
Primary authority for the prescribing of legend drugs and controlled substances comes from individual professional practice acts, usually in the section of the act which defines the scope of practice for the profession. The definition of scope of practice is the responsibility of the board that licenses the professional. Only those providers not excluded by federal programs are eligible.
DUR Board
The Drug Use Review (DUR) Board performs drug utilization review and educational interventions. Five pharmacists and four physicians comprise the DUR Board which is coordinated by a full-time registered Montana pharmacist. The DUR Board meets monthly to review utilization and advise the Department.
Drug Use Review (DUR) Board meetings are posted on the Provider website. On the Pharmacy page, click on the Drug Use Review (DUR) Board pane.
The DUR Board and The University of Montana Skaggs School of Pharmacy also advise the Department on its outpatient drug formulary. Drugs are evaluated for safety, effectiveness, and clinical outcome. Drugs recommended for formulary exclusion have no significant, clinically meaningful therapeutic advantage over drugs recommended for inclusion.
End of Drug Program Chapter
Montana Healthcare Programs Covered Products
What Drugs and Pharmaceutical Supplies Are Covered?
Drug coverage is limited to those products where the pharmaceutical manufacturer has signed a rebate agreement with the federal government. Federal regulations further allow states to impose restrictions on payment of prescription drugs through prior authorization and preferred drug lists (PDL).
The Montana Healthcare Programs Prescription Drug Program covers the following:
- Legend drugs, subject to the PDL and prior authorization requirements.
- Selective non-prescription (over the counter (OTC)) medications. See the OTC Coverage tab on the Pharmacy page of the website. Nursing facilities are responsible for providing OTC antacids, aspirin, and laxatives to their residents.
- Compounded prescriptions
- Contraceptive supplies and devices
- Federal law allows states the discretion to cover certain medications listed in 42 USC 1396r-8. Montana Healthcare Programs has opted to cover the following medications for all members, including Medicare Part D members:
- Prescription cough and cold medications
- Selective non-prescription (over the counter (OTC)) medications. See the OTC Coverage tab on the Pharmacy page of the website. Montana Healthcare Programs does not cover proton pump inhibitors or non-sedating antihistamines for Part D members when the member’s prescription drug plan covers these classes of drugs.
- Vitamins and minerals may be granted prior authorization when indicated for the treatment of an appropriate diagnosis.
What Drugs and Pharmaceutical Supplies Are Not Covered?
The Montana Healthcare Programs Prescription Drug Program does not reimburse for the following items or services:
- Drugs supplied by drug manufacturers who have not entered into a federal drug rebate agreement.
- Drugs supplied by other public agencies such as the United States Veterans Administration, United States Department of Health and Human Services, local health departments, etc.
- Drugs for Medicare Part D dual eligible members, except for drugs covered in #5 in the What Drugs and Pharmaceutical Supplies Are Covered? section above.
- Drugs prescribed:
- To promote fertility
- For erectile dysfunction
- For weight reduction
- For cosmetic purposes or hair growth
- For an indication that is not medically accepted as determined by the Department in consultation with federal guidelines, the DUR Board, or the Department medical and pharmacy consultants.
- Drugs designated as less-than-effective (DESI drugs) or drugs that are identical, similar, or related to such drugs.
- Drugs that are experimental, investigational, or of unproven efficacy or safety.
- Free pharmaceutical samples.
- Obsolete National Drug Code (NDC).
- Terminated drug products.
- Any drug, biological product, or insulin provided as part of, or incident to and in the same setting as, any of the following:
- Inpatient hospital setting
- Hospice services
- Outpatient hospital services emergency room visit
- Other laboratory and x-ray services
- Renal dialysis
- Incarceration
- Any of the following drugs:
- Outpatient nonprescription drugs (except those OTC products previously listed)
- Covered outpatient drugs for which the manufacturer seeks to require as a condition of sale that associated tests or monitoring services be purchased exclusively from the manufacturer or its designee.
- Medical supplies (non-drug items) are not covered under the Prescription Drug Program.
a. Exception: Contraceptive supplies and devices
The Montana Preferred Drug List
To address the rising costs of prescription drugs, Montana Healthcare Programs implemented a preferred drug list (PDL) in 2005. The Department of Public Health and Human Services uses this program to provide clinically effective and safe drugs to its members at the best available price.
The PDL addresses certain classes of medications and provides a selection of therapeutically effective products for which the Montana Healthcare Programs will allow payment without restriction in those targeted classes. The Department, through its Formulary Committee, designates this listing of preferred drugs as “preferred” based primarily on clinical efficacy. In the designated classes, drug products that are non-preferred on the PDL will require prior authorization.
The Department updates the PDL annually and periodically as new drugs and information become available.
The current Montana PDL can be found on the Preferred Drug Information tab on the Pharmacy Page of the Provider Information website. Providers may address questions regarding the PDL and requests for prior authorization to the Drug Prior Authorization Unit. (See the Key Contacts chapter) The PDL/Prior Authorization Help Line is for providers only. Montana Healthcare Programs members with questions can ask their providers or call the Member Help Line, (800) 362-8312.
Medicare Part B and Part D Drug Claims
Part D
Medicare added prescription drug coverage for its beneficiaries under the Medicare Modernization Act, 42 USC 1302 Sec. 1395. Members enrolled in Medicare Part A and/or Part B are eligible for Medicare Part D and are required to receive their drug benefits through a Medicare Prescription Drug Plan (PDP). Members enrolled in both Montana Healthcare Programs and Medicare are considered “dual eligible” and are auto-enrolled in a Medicare PDP if they do not choose a plan. The Montana Healthcare Programs reimbursement for outpatient drugs provided to a full-benefit dual eligible member will be limited to the excluded drugs identified in this chapter and the Part B drugs described in the following paragraph.
Part B
Claims cross over automatically if the provider’s NPI/API is on file with Montana Healthcare Programs. The taxonomy code for the pharmacy is required on the claim.
To bill paper claims:
- Submit your claims on a CMS-1500 form.
- Attach the Medicare EOMB.
- Use your NPI/API.
- Mail to the Claims Processing Unit, P.O. Box 8000, Helena, MT 59604.
- Providers using paper claims must wait 45 days after Medicare paid date to submit claims.
Part B Crossover Claims
Part B crossover claims will be reimbursed using the following “lower of” pricing methodology:
- Montana Healthcare Programs allowed minus the Medicare paid; or
- Medicare coinsurance plus Medicare deductible.
Montana Healthcare Programs allowed for the pharmacy supplying and dispensing fee is $4.94.
For an updated list of covered Part B drugs, visit the CMS website, https://www.cms.gov.
End of Montana Healthcare Programs Covered Products Chapter
Dispensing Limitations
Prescription Quantity (ARM 37.86.1102)
Medications may not be dispensed in quantities greater than a 34-day supply except where manufacturer packing cannot be reduced to a smaller quantity.
1. The following drug classes, with examples, are considered maintenance medications and may be dispensed up to a 90-day supply.
Drug Classes Considered for Maintenance Medications
Cardiovascular (Heart Health)
- Antiarrhythmics — digoxin, amiodarone
- Antihypertensives (Blood Pressure)
- Angiotensin Modulators and Combinations — benazepril, lisinopril, irbesartan, losartan, valsartan, losartan/HCTZ, valsartan/HCTZ, lisinopril/HCTZ, enalapril/HCTZ
- Calcium Channel Blockers and Combinations — amlodipine, nifedipine, verapamil, diltiazem, amlodipine/valsartan, amlodipine/benazepril, Exforge HCT
- Beta Blockers and Alpha Blockers — atenolol, propranolol, metoprolol, prazosin, doxazosin, terazosin, carvedilol
- Alpha Agonists — clonidine, guanfacine, methyldopa
- Vasodilators — hydralazine, minoxidil, isosorbide
- Diuretics — furosemide, bumetanide, torsemide, HCTZ, metolazone, chlorothiazide, indapamide, spironolactone, amiloride, triamterene/HCTZ, spironolactone/HCTZ, amiloride/HCTZ
- Antihyperlipidemics (Cholesterol) — atorvastatin, lovastatin, pravastatin, rosuvastatin, simvastatin, gemfibrozil, fenofibrate, ezetimibe
- Platelet Aggregation inhibitors and hemorrhelogic agents (Blood Thinners) — Aggrenox, aspirin, clopidogrel, dipyridamole, Effient, Brillinta, pentoxifylline
Diabetes
- Antihyperglycemic — glimepiride, glipizide, glyburide, metformin, acarbose, Glyset, glyburide/metformin
Central Nervous System
- Anticonvulsants (exclusions apply) — divalproex, ethosuximide, phenytoin, lamotrigine, levetiracetam, topiramate, zonisamide, carbamazepine, oxcarbazepine
- Anti-Parkinson's and Other Movement Disorders — carbidopa, amantadine, pramipexole, ropinirole, carbidopa-levodopa
- Skeletal Muscle Relaxants — baclofen, chlorzoxazone, cyclobenzaprine, methocarbamol, orphenadrine, tizanidine
Gastrointestinal
- Antacids — Tums, Maalox
- Anti-Ulcer — sucralfate, misoprostol
- H2-Inhibitors — famotidine, ranitidine
- Bile Salts — ursodiol
Renal System
- Incontinence — oxybutynin, Toviaz
- Electrolyte Depleters/Replacers — calcium acetate, Renagel, potassium chloride, Phos-Nak, potassium citrate
- Hyperuricemia (Gout) — allopurinol, probenecid
Respiratory
- Antihistamines — cetirizine, loratadine, levocetirizine
- Leukotriene Receptor Antagonist (Asthma/Allergies) — montelukast
- Other — theophylline
Men and Women’s Health
- Contraceptives (oral, transdermal, intravaginal)
- Prostate — alfuzosin, tamsulosin, finasteride, dutasteride
- Breast Cancer — tamoxifen
- Vitamin Supplementation (restrictions apply) — prenatal vitamins, vitamin B, vitamin D, folic acid
Other Body Systems
- Bone Strength — alendronate, raloxifene
- Thyroid/Antithyroid — levothyroxine, methimazole, propylthiouracil
- NSAIDs (Pain/Inflammation) — diclofenac, ibuprofen, indomethacin, meloxicam, naproxen, sulindac, celecoxib
2. No more than two prescriptions of the same drug may be dispensed in a calendar month except for the following:
- Antibiotics
- Schedule II through V drugs
- Antineoplastic agents
- Compounded prescriptions
- Prescriptions for suicidal members or members at risk for drug abuse
- Topical preparations
The DUR Board has set monthly limits on certain drugs. Use over these amounts requires prior authorization.
Prescription Refills
Prescriptions for non-controlled substances may be refilled after 75% of the estimated therapy days have elapsed. Prescriptions for controlled substances (CII-CV), Ultram (tramadol), Ultracet (tramadol/acetaminophen), carisoprodol, and gabapentin may be refilled after 90% of the estimated therapy days have elapsed. The POS system will deny a claim for “refill to soon” based on prescriptions dispensed on month-to-month usage.
A prescription may be refilled early only if the prescriber changes the dosage, or if the member was admitted to a nursing facility. The pharmacist must document any dosage change. In any circumstance, the provider must contact the Drug Prior Authorization Unit to receive approval. (See Key Contacts.)
Pharmacists who identify members who experience difficulties in managing their drug therapy may consider unit dose prescriptions (see below).
Generic Drugs
The Department has a mandatory generic edit in the claims processing system. The edit is enabled once there are two rebateable AB-rated generic drugs available in the marketplace. Typically, the first generic labeler will have a six-month period of market exclusivity. To maximize value to the State, the Department recommends dispensing the brand name drug over the generic during this period of market exclusivity. Brands may be preferred over generics in other instances where there is a net cost benefit to the Department. Brand over generic preferences are listed on the PDL. When there are “preferred brands” on the Department’s PDL, generic equivalent drugs will require a prior authorization.
For drugs not subject to PDL restrictions and for those drugs listed in the Dispense As Written (DAW) section of the Billing Procedures chapter, if the brand name drug is prescribed instead of a generic equivalent, the prescriber must get prior authorization.
Authorization is based on medical need such as adverse reactions or therapeutic failures (clinically demonstrated, observed and documented) which have occurred when the generic drug has been used.
Unit Dose Prescriptions
Pharmacy-packaged unit dose medications may be used to supply drugs to members in nursing facilities, group homes, and other institutional settings.
Members who are not in one of the above facilities may also be considered high-risk and eligible for unit dose packaging if they:
- Have one or more of the following representative disease conditions: Alzheimer’s disease, blood clotting disorders, cardiac arrhythmia, congestive heart failure, depression, bipolar, cancer, diabetes, epilepsy, HIV/AIDS, hypertension, schizophrenia, or tuberculosis; and
- Consume two or more prescribed concurrent chronic medications which are dosed at three or more intervals per day; or
- Have demonstrated a pattern of noncompliance that is potentially harmful to their health.
Unit dose prescriptions may not exceed the 34-day supply limit.
Compounding
The Department shall reimburse pharmacies for compounding drugs only if the member’s drug therapy needs cannot be met by commercially available dosage strengths and/or forms of the therapy.
Prescription claims for compound drugs shall be billed and reimbursed using the National Drug Code (NDC) number and quantity for each compensable ingredient in the compound. No more than 25 ingredients may be reimbursed in any compound. Reimbursement for each drug component shall be determined in accordance with ARM 37.86.1101. Prior authorization requirements for individual components of a compound must be met for reimbursement purposes. The Department does not consider reconstitution to be compounding.
The Department may reimburse for compounded non-rebateable API bulk powders and excipients on the Department’s drug formulary maintained in accordance with ARM 37.86.1102.
End of Dispensing Limitations Chapter
Prior Authorization
Prior Authorization for Covered Drugs
Many drug products require prior authorization before the pharmacist provides them to the member. Requests are reviewed for medical necessity.
- Grandfathering of medications does not apply if samples, patient assistance, or cash pay have been used to bypass criteria or Preferred Drug List (PDL) placement.
- To request prior authorization, providers must submit the necessary information to the Drug Prior Authorization Unit. See the Pharmacy Resources page on the Mountain Pacific website.
- The prescriber (e.g., physician) or pharmacy may submit requests by mail, telephone, or fax to:
Drug Prior Authorization Unit
Mountain Pacific
P.O. Box 5119
Helena, MT 59604
(406) 443-6002 or 800-395-7961 (Phone)
(406) 513-1928 or 800-294-1350 (Fax)
- Requests are reviewed and decisions made immediately in most cases. Decisions on requests with special circumstances that require further peer review are made within 24 hours. Requests received after the Drug Prior Authorization Unit’s regular working hours of 8 a.m. to 5 p.m., Monday through Friday, or on weekends or holidays, are considered received at the start of the next working day.
- An emergency 72-hour supply may be dispensed for emergency, after-hours, weekend, and holiday requests. Payment will be authorized by using a “3” in the Days Supply field and a value of “8” in the Prior Authorization Type Code field.
Prior Authorization for Retroactively Eligible Members
All prior authorization requirements must be met for retroactively eligible members.
When a member is determined retroactively eligible for Montana Healthcare Programs, the member should give the provider a Notice of Retroactive Eligibility (160-M).
The provider has 12 months from the date retroactive eligibility was determined to bill for those services.
Retroactive Montana Healthcare Programs eligibility does not allow a provider to bypass prior authorization requirements.
When a member becomes retroactively eligible for Montana Healthcare Programs, the provider may:
- Accept the member as a Montana Healthcare Programs member from the current date.
- Accept the member as a Montana Healthcare Programs member from the date retroactive eligibility was effective.
- Require the member to continue as a private-pay member.
Providers may choose whether to accept retroactive eligibility. (See the General Information for Providers Manual, Member Eligibility and Responsibilities chapter.) All prior authorization requirements must be met to receive Montana Healthcare Programs payment.
When submitting claims for retroactively eligible members, attach a copy of the Notice of Retroactive Eligibility (Form 160-M) to the claim if the date of service is more than 12 months earlier than the date the claim is submitted.
End of Prior Authorization Chapter
Reimbursement
Reimbursement for Covered Drugs
Reimbursement for covered brand and generic preferred drugs shall not exceed the lowest of:
- The provider’s usual and customary charge of the drug to the general public; or
- The allowed ingredient cost plus a professional dispensing fee. Where allowed ingredient cost is defined as the lower of:
- The Average Acquisition Cost (AAC); or
- Submitted ingredient cost.
- If an AAC rate is not available, drug reimbursement is determined at the lower of:
- Wholesale Acquisition Cost (WAC);
- Affordable Care Act Federal Upper Limit (ACA FUL); or
- Submitted ingredient cost.
Average Acquisition Cost
Average acquisition cost (AAC) is the calculated average drug ingredient cost per drug determined by direct pharmacy survey, wholesale survey, and other relevant cost information. The AAC rates are published online under the Pharmacy Provider webpage.
Submitted Ingredient Cost
Submitted Ingredient is a pharmacy’s actual ingredient cost. For drugs purchased under the 340B Drug Pricing Program, submitted ingredient cost means the actual 340B purchase price. For drugs purchased under the Federal Supply Schedule (FSS), submitted ingredient cost means the actual FSS purchase price.
Usual and Customary
The usual and customary charge is the price the provider most frequently charges the general public for the same drug. In determining “usual and customary” prices, the Department:
- Does not include prescriptions paid by third party payers, including health insurers, governmental entities, and Montana Healthcare Programs, in the general public.
- Includes discounts advertised or given (including but not limited to cash rebate, monetary price discount, coupon of value) to any segment of the general public.
- Uses the lower of the two pricing policies if a provider uses different pricing for “cash” and “charge” members.
- Will use the median price if during an audit, the most frequent price cannot be determined from pharmacy records.
Federal Maximum Allowable Cost (MAC)
- The Federal Upper Limit pricing set by the U.S. Department of Health and Human Services Centers for Medicare & Medicaid (CMS).
Dispensing Fee
- The dispensing fee assigned shall range between:
- The minimum of $4.11 and the maximum of $17.52 for pharmacies with an annual prescription volume between 0 and 39,999
- The minimum of $4.11 and the maximum of $15.17 for pharmacies with an annual prescription volume between 40,000 and 69,999; or
- The minimum is $4.11 and the maximum is $12.83 for pharmacies with an annual prescription volume greater than 70,000.
- The dispensing fee for each compounded drug shall be $12.50, $17.50, or $22.50 based on the level of effort required by the pharmacist.
- New pharmacy providers are assigned the maximum dispensing fee. Failure to comply with the six-month dispensing fee questionnaire requirement will result in assignment of a dispensing fee of the lowest calculated cost to dispense that year.
- Pharmacies may receive an additional $0.75 for dispensing pharmacy-packaged unit dose prescriptions.
- Dispensing fee surveys are available from the Department of Public Health and Human Services Prescription Drug Program. (See Key Contacts.)
Vaccine Administration Fee
Pharmacies can receive a vaccine administration fee. This fee is in lieu of the standard dispensing fee. The fee for the first vaccine administered will be $21.32; the fee for each additional vaccine administered will be $16.04.
For the COVID-19 vaccine, Montana Healthcare Programs will follow the Medicare established rates for the administration fee, which are different from the above rates.
The Remittance Advice
The remittance advice is the best tool providers have to determine the status of a claim. Remittance advices accompany payment for services rendered. The remittance advice provides details of all transactions that have occurred during the previous remittance advice cycle. Each line of the remittance advice represents all or part of a claim and explains whether the claim or service has been paid, denied, or suspended (also referred to as pending). If the claim was suspended or denied, the remittance advice also shows the reason. See the General Information for Providers Manual for more information on the remittance advice.
As of July 2013, all new providers were required to enroll in electronic funds transfer (EFT) and receive electronic remittance advices. Providers who enrolled prior to July 2013 who received paper checks or paper remittance advices were transitioned to the electronic-only system over time.
Credit Balances
Credit balances occur when claim adjustments reduce original payments causing the provider to owe money to the Department. These claims are considered in process and continue to appear on the remittance advice until the credit has been satisfied. Credit balances can be resolved in two ways:
- By working off the credit balance. Remaining credit balances can be deducted from future claims. These claims will continue to appear on consecutive remittance advices until the credit has been paid.
- By sending a check payable to DPHHS for the amount owed. This method is required for providers who no longer submit claims to Montana Healthcare Programs. Attach a note stating that the check is to pay off a credit balance and include your provider number. Send the check to Third Party Liability
Rebilling and Adjustments
Rebillings and adjustments are important steps in correcting any billing problems you may experience. Knowing when to use the rebilling process versus the adjustment process is important. When submitting a reversal (void) use a B2 NCPDP transaction and when submitting a rebilled claim or an adjustment use a B3 NCPDP transaction (void & rebill).
Timeframe for Rebilling or Adjusting a Claim
- Providers may resubmit or adjust any initial claim within the timely filing limits described in the Billing Procedures chapter of this manual. Depending on switch-vendor requirements, some point-of-sale adjustments must be completed within three months. In this case, adjustments may be submitted on paper within the timely filing limits.
- These time periods do not apply to overpayments that the provider must refund to the Department. After the 12-month time period, a provider may not refund overpayments to the Department by completing a claim adjustment. The provider may refund overpayments by issuing a check or asking the Third-Party Liability Unit to complete a gross adjustment.
Rebilling Montana Healthcare Programs
Rebilling is when a provider submits a claim or claim line to Montana Healthcare Programs that was previously submitted for payment but was either returned or denied. Pharmacy providers can rebill Montana Healthcare Programs via point-of-sale or on paper. Paper claims are often returned to providers before processing because information such as the NPI or authorized signature/date are missing or unreadable. See the Billing Procedures chapter for tips on preventing returned or denied claims.
When to Rebill Montana Healthcare Programs
- Claim Denied. Providers can rebill Montana Healthcare Programs when a claim is denied in full, as long as the claim was denied for reasons that can be corrected. When the entire claim is denied, check the Explanation of Benefits (EOB) code, make the appropriate corrections, and resubmit the claim (not an adjustment).
- Line Denied. When an individual line is denied on a multiple-line claim, correct any errors and rebill Montana Healthcare Programs. Either submit the denied service on a new Universal Claim Form Version 1.2-02/2013, or cross out paid lines and resubmit the form, or submit via point-of-sale. Do not use an adjustment form.
- Claim Returned. Rebill Montana Healthcare Programs when the claim is returned under separate cover. Occasionally, Montana Healthcare Programs is unable to process the claim and will return it to the provider with a letter stating that additional information is needed to process the claim. Correct the information as directed and resubmit your claim. Paper pharmacy claims should be billed on a Universal Claim Form Version 1.2-02/2013.
How to Rebill
- Check any EOB code listed and make your corrections on a copy of the claim, or produce a new claim with the correct information, or rebill using point-of-sale.
- When making corrections on a copy of the claim, remember to cross out or omit all lines that have already been paid. The claim must be neat and legible for processing.
- Enter any insurance (third party liability) information on the corrected claim, or attach insurance denial information to the corrected claim, and send it to Claims Processing.
Adjustments
If a provider believes that a claim has been paid incorrectly, the provider may call Provider Relations. Once an incorrect payment has been verified, the provider may submit an Individual Adjustment Request form to Provider Relations or submit an adjustment through point-of-sale. If incorrect payment was the result of a Conduent keying error, the provider should contact Provider Relations.
When adjustments are made to previously paid claims, the Department recovers the original payment and issues appropriate repayment. The result of the adjustment appears on the provider’s RA as two transactions. The original payment will appear as a credit transaction. The replacement claim reflecting the corrections will be listed as a separate transaction and may or may not appear on the same remittance advice as the credit transaction. The replacement transaction will have nearly the same ICN number as the credit transaction, except the 12th digit will be a 2, indicating an adjustment. Adjustments are processed in the same time frame as claims.
When to Request an Adjustment
- • Request an adjustment when a claim was overpaid or underpaid.
• Request an adjustment when a claim was paid but the information on the claim was incorrect (e.g., member ID, NPI, date of service, NDC, prescribing provider, units).
How to Request an Adjustment
To request an adjustment, use the Individual Adjustment Request form. Adjustments may also be made using point-of-sale. The requirements for adjusting a claim are as follows:
- Claims Processing must receive individual claim adjustment requests within 12 months of the date of service. (See Timely Filing Limits in the Billing Procedures chapter.) After this time, gross adjustments are required.
- Use a separate adjustment request form for each TCN.
- If you are correcting more than one error per TCN, use only one adjustment request form, and include each error on the form.
- If more than one line of the claim needs adjusting, indicate which lines and items need to be adjusted in the Remarks section of the adjustment form.
Completing an Adjustment Request Form
- You may download the Individual Adjustment Request form from the Provider Information website. Complete Section A first with provider and member information and the claim’s TCN.
- Complete Section B with information about the claim. Complete only the items that need to be corrected. (See the table on next page.)
- Enter the date of service or the line number in the Date of Service or Line Number column.
- Enter the information from the claim that was incorrect in the Information on Statement column.
- Enter the correct information in the Corrected Information column.
- Attach copies of the remittance advice and a corrected claim if necessary.
- If the original claim was billed electronically, a copy of the remittance advice will suffice.
- If the remittance advice is electronic, attach a screen print of it.
- Verify the adjustment request has been signed and dated.
- Send the adjustment request to Claims Processing.
- If an original payment was an underpayment by Montana Healthcare Programs, the adjustment will result in the provider receiving the additional payment amount allowed.
- If an original payment was an overpayment by Montana Healthcare Programs, the adjustment will result in recovery of the overpaid amount through a credit balance or a check from the provider. (See Credit Balances earlier in this chapter.)
- Any questions regarding claims or adjustments must be directed to Provider Relations.
Completing an Individual Adjustment Request Form
Section A
Field: 1. Provider Name and Address
Description: Provider’s name and address (and mailing address if different).
Field: 2. Member Name
Description: The member’s name.
Field: 3.* Internal Control Number (ICN)
Description: There can be only one TCN per Adjustment Request form. When adjusting a claim that has been previously adjusted, use the TCN of the most recent claim.
Field: 4*. Provider NPI/API
Description: The provider’s NPI/API
Field: 5*. Member's Montana Healthcare Programs Number
Description: Member's Montana Healthcare Programs ID number.
Field: 6. Date of Payment
Description: Date claim was paid found on Remittance Advice Field 5 (see the sample RA earlier in this chapter).
Field: 7. Amount of Payment
Description: The amount of payment from the Remittance Advice Field 19 (see the sample RA earlier in this chapter.).
Section B
Field: 1. Units of Service
Description: If a payment error was caused by an incorrect number of units, complete this line.
Field: 2. Procedure Code/NDC/Revenue Code
Description: If the procedure code, NDC, or revenue code are incorrect, complete this line.
Field: 3. Dates of Service (DOS)
Description: If the date of service is incorrect, complete this line.
Field: 4. Billed Amount
Description: If the billed amount is incorrect, complete this line.
Field: 5. Personal Resource (Nursing Facility)
Description: If the member's personal resource amount is incorrect, complete this line.
Field: 6. Insurance Credit Amount
Description: If the member’s insurance credit amount is incorrect, complete this line.
Field: 7. Net (Billed - TPL or Medicare Paid)
Description: If the payment error was caused by a missing or incorrect insurance credit, complete this line. Net is billed amount minus the amount TPL or Medicare paid.
Field: 8. Other/Remarks
Description: If none of the above items apply, or if you are unsure what caused the payment error, complete this line.
*Indicates a required field
Mass Adjustments
Mass adjustments are done when it is necessary to reprocess multiple claims. They generally occur when:
- Montana Healthcare Programs has a change of policy or fees that is retroactive. In this case federal laws require claims affected by the changes to be mass adjusted.
- A system error that affected claims processing is identified.
Providers are informed of mass adjustments by a provider notice or on the first page of the remittance advice. Mass adjustment claims shown on the RA have an ICN that begins with a 4.
Payment and the Remittance Advice
Providers receive their Montana Healthcare Programs payment and remittance advices weekly. To sign up for EFT (direct deposit) and register for the web portal to view or download remittance advices, providers need to complete the EFT and ERA Authorization Agreement and the EDI Trading Partner Agreement and mail or fax them to Provider Relations. See the Provider Enrollment page for those documents.
A letter from your financial institution verifying legitimacy of the account is also required. The letter must include the name and contact information of the bank representative and be signed by the bank representative. Do not send voided checks or deposit slips.
Once enrolled in EFT and registered for the MATH web portal, providers are able to receive their electronic remittance advices. Due to space limitations, each remittance advice is available on the web portal for 90 days.
For assistance on enrolling in EFT, completing the EDI Trading Partner Agreement, and registering for the MATH web portal, contact Provider Relations.
End of Reimbursement Chapter
Billing Procedures
How to Bill Pharmacy Claims
- The Department supports NCPDP X2 Version D.0 electronic transactions.
- If a claim must be billed on paper, the Department supports the Universal Claim Form Version 1.2 - 02/2013.
- Pharmacies are eligible to receive five free Universal Claim Forms per year through NCPDP. To obtain a copy, please call (480) 477-1000.
- If a pharmacy needs more paper forms, they can be ordered through CommuniForm LLC via phone (877) 817-3676 or fax at (866) 308-2036. Providers may also request online login access from CommuniForm LLC by calling (877) 817-3676 to order forms online.
- Pharmacies are eligible to receive five free Universal Claim Forms per year through NCPDP. To obtain a copy, please call (480) 477-1000.
Provider Number
- The Department uses the pharmacy’s NPI as the provider number for billing purposes.
- The Department-assigned provider number is used for payment and reporting purposes.
- Changes in pharmacy ownership or NABP (NCPDP) number must be reported immediately to ensure that payments are received by the billing owner. Contact Provider Relations to report all ownership changes.
Provider Enrollment
P.O. Box 4936
Helena, MT 59604
(800) 624-3958
(406) 442-1837
Tamper-Resistant Pads
Written prescriptions must contain all of the following.
- One or more industry-recognized features designed to prevent unauthorized copying of a completed or blank prescription form;
- One of more industry-recognized features designed to prevent the erasure or modification of information written on the prescription by the prescriber; and
- On or more industry-recognized features designed to prevent the use of counterfeit prescription forms.
Outpatient pharmacy claims for Montana Healthcare Programs require the prescription origin code to indicate the source of the prescription. Valid values for prescription origin code are:
- 0 – Not specified
- 1 – Written prescription
- 2 – Telephone
- 3 – Electronic
- 4 – Facsimile
How Long Do I Have to Bill?
Providers are required to submit a clean claim no later than 365 days from:
- The date of service;
- The date retroactive eligibility is determined;
- The date disability is determined; or
- Within 6 months of the date Medicare pays, whichever is later.
A clean claim is one that can be adjudicated without correction or additional information or documentation from the provider.
Prescription Tracking and Claim Reversals
For purposes of billing for prescribed drugs, the date of service means the date a prescription is filled. If the drug has not been received by the member or the member’s representative within 15 days after the prescription is filled, the pharmacy must reverse the claim and refund the payment to the Department.
Tips to Avoid Timely Billing Denials
- Correct and resubmit denied claims promptly. (See the Reimbursement chapter, Remittance Advices and Adjustments section in this manual.)
- If a claim submitted to Montana Healthcare Programs does not appear on the remittance advice within 30 days, contact Provider Relations for claim status.
When to Bill Montana Healthcare Programs Members (ARM 37.85.406)
In most circumstances, providers may not bill Montana Healthcare Programs members for services covered under Montana Healthcare Programs. More specifically, providers cannot bill members directly:
- For the difference between charges and the amount Montana Healthcare Programs paid.
- For a covered service provided to a Montana Healthcare Programs-enrolled member who was accepted as a Montana Healthcare Programs member by the provider, even if the claim was denied.
Under certain circumstances, providers may need a signed agreement in order to bill a Montana Healthcare Programs member (see the following table).
Routine Agreement: This may be a routine agreement between the provider and member which states that the member is not accepted as a Montana Healthcare Programs member, and that he/she must pay for the services received.
Custom Agreement: This agreement lists the service the member will receive and states that the service is not covered by Montana Healthcare Programs and that the member will pay for the services received.
Billing for Retroactively Eligible Members
When the provider accepts the member’s retroactive eligibility, the provider has 12-months from the date retroactive eligibility was determined to bill for those services.
When submitting claims for retroactively eligible members in which the date of service is more than 12 months earlier than the date the claim is submitted, attach a copy of the Provider Notice of Eligibility (Form 160-M). The provider must request the form from the member’s local Office of Public Assistance.
See the DPHHS Field Offices Public Assistance webpage. For more information on retroactive eligibility, see the Member Eligibility and Responsibilities chapter in the General Information for Providers Manual.
Usual and Customary Charge (ARM 37.85.406)
Providers should bill Montana Healthcare Programs their usual and customary charge for each service; that is, the same charge that is made to other payers for that service.
Member Co-Payment (ARM 37.85.204)
Effective for all claims paid on or after January 1, 2020 co-payment will not be assessed.
The provider must always use the complete 11-digit NDC from the dispensing container.
National Drug Codes (NDC)
All outpatient prescription drugs are billed using the drug’s NDC, the 11-digit code assigned to all prescription drug products by the labeler or distributor of the product under FDA regulations.
The Department accepts only the 5-4-2 NDC format. All 11 digits, including zeros, must be entered. The three segments of the NDC are:
SAMPLE NDC: 12345-6789-10
12345 = labeler code
6789 = product code
10 = package size
Claims must accurately report the NDC dispensed, the number of units dispensed, days supply, and the date of dispensing. Use of an incorrect NDC or inaccurate reporting of a drug quantity will cause the Department to report false data to drug manufacturers billed for drug rebates.
The Department will recover payments made on erroneous claims discovered during dispute resolution with drug manufacturers. Pharmacies are required to document purchase for quantities of brands of drugs reimbursed by the Department if disputes occur.
Dispense As Written (DAW)
Prescribers and pharmacies must prescribe and dispense the generic form of a drug whenever possible. Except for those drugs listed below, prior authorization is required when a brand name drug is prescribed instead of a generic equivalent. Please use the following DAW codes for these situations:
- DAW 1 may only be used if authorized by the Drug Prior Authorization Unit. In addition to prior authorization requirements, brand name drugs with a generic equivalent (except those required by the PDL) may be billed only when the prescriber has handwritten “brand necessary” or “brand required” on the prescription. The pharmacy must retain brand certifications as documentation.
- DAW 5 may be used in instances where the drug dispensed is generic but is listed as a brand (branded generics) and some cases a prior authorization is required.
- DAW 7 may be used for seizure medications with an appropriate diagnosis without prior authorization. Based on DUR Board recommendations only antiepileptic medications being used for a seizure diagnosis, and anti-hemophilic factors will continue to be considered narrow therapeutic index (NTI) drugs. A DAW 7 override will be allowed on these drugs only. See the 2009 provider notice on the Pharmacy page of the website for additional information.
- DAW 9 is used when a brand name multisource drug is preferred and pharmacy is dispensing the brand name drug, this exempts the pharmacy from using the generic and allows reimbursement at the brand name rate.
Abuse and Misutilization
The following practices constitute abuse and misutilization:
- Excessive Fees: Commonly known as prescription splitting or incorrect or excessive dispensing fees. Billing inappropriately in order to obtain dispensing fees in excess of those allowed by:
- Supplying medication in amounts less than necessary to cover the period of the prescription.
- Supplying multiple medications in strengths or quantities less than those prescribed to gain more than one dispensing fee.
- Excessive Filling: Billing for an amount of a drug or supply greater than the prescribed quantity.
- Prescription Shorting: Billing for drug or supply greater than the quantity actually dispensed.
- Substitution to Achieve a Higher Price: Billing for a higher priced drug than prescribed even though the prescribed lower priced drug was available.
Third Party Payer – Negative Payment Amounts
Montana Healthcare Programs will not approve a claim with a negative payment amount (from click fees or PBM clawbacks) or allow pharmacies to bypass the primary insurance to eliminate the negative payment amount. If a pharmacy receives a negative amount from the primary insurance and a member has Montana Healthcare Programs as secondary, the pharmacy must bill with the following to receive payment from the Department:
- Other Coverage Code = 4, defined as Other Coverage exists – payment not collected – NCPDP field (308-C8)
- Other Payer Amount – NCPDP field (431-DV) = $0.00
In addition, providers are reminded that aside from a member copayment, if there is one, payment from Montana Healthcare Programs is payment in full. Negative payment amounts may not be passed on to members.
Psychiatric Residential Treatment Facility (PRTF) Non-Psychotropic Medications
Pharmacies who fill medications for PRTFs are able to bill for non-psychotropic medications for members currently in an all-inclusive PRTF by submitting the claim with a submission clarification code (SCC) of 10 in NCPDP field (420-DK). If these pharmacies receive a claim rejection of “member enrolled in all-inclusive program, contact facility for payment” despite submitting with a SCC code of 10, this indicates the medication being billed is classified as a psychotropic medication and can’t be reimburse through the pharmacy benefit. Psychotropic medications are included in the all-inclusive payment and must be billed to the facility. However, if the medication is on the psychotropic list but is being used for a non-psychiatric diagnosis, a prior authorization may be obtained by calling the Drug Prior Authorization Unit at (406) 443-6002 or (800) 395-7961.
If pharmacies are trying to bill prescriptions for a member that has been released from an all-inclusive facility but are still getting denied claims with the same rejection referenced above, please contact the Pharmacy Program Officer or the Montana Healthcare Programs Pharmacist.
End of Billing Procedures Chapter
Point-of-Sale
What Is the Pharmacy Point-of-Sale (POS)?
The point-of-sale (POS) system finalizes claims at the point of entry as either paid or denied. Pharmacies arrange their own telecommunications switch services to accept Montana Healthcare Programs point of sale and are responsible for any charges imposed by these vendors. Hard copy (paper) billing is still accepted when billed on a Universal Claim Form Version 1.2-02/2013. All claims are processed and edited through the POS system regardless of how the claim was originally submitted.
If the claim continues to deny for eligibility past 3 working days, call Provider Relations at (800) 624-3958.
Possession of a Montana Access to Health (MATH) Montana Healthcare Programs ID card is not proof of eligibility.
Member eligibility may change monthly, so providers should verify eligibility each month. Both the 7-digit member number and the member’s Social Security number are billable numbers. If a claim is rejected online, a provider should verify eligibility by one of the methods (MATH web portal, IVR, FaxBack, calling Provider Relations) described in the General Information for Providers Manual.
Pro-DUR
The POS system performs all major prospective drug utilization review (Pro-DUR) edits. In some circumstances, the Pro-DUR edits result in denied claims. When a Pro-DUR denied claim needs to be overridden, pharmacy providers may enter one Reason for Service Code (formerly DUR Conflict Code) from each category in the following order, as long as the indicated situations exist and the pharmacy retains documentation in its files:
- Two-byte alpha Reason for Service Code, followed by...
- Two-byte alphanumeric Professional Service Code, followed by...
- Two-byte alphanumeric Result of Service Code
By placing codes into the claim, the provider is certifying that the indicated DUR code is true and documentation is on file. For questions regarding DUR codes, contact the Drug Prior Authorization Unit.
NCPDP DUR Codes
End of Point-of-Sale Chapter
Billing a Paper Claim
Completing a Universal Claim Form
Providers may also request online login access from CommuniForm LLC by calling (877) 817-3676. Forms can be ordered online by logging in on the Welcome page of the ACES Benefits website
Paper claims must be mailed to the following address:
Claims Processing Unit
P.O. Box 8000
Helena, MT 59604
Universal Claim Form Instructions
| Field Number | Field Title | Instructions |
|---|---|---|
| 1 | ID-Insurance | Enter the Member ID. |
| 2 | Group ID-Insurance | Enter the insurance Group ID. |
| 3 | Last-Insurance | Enter the last name of the member |
| 4 | First-Insurance | Enter the first name of the member. |
| 5 | Plan Name-Insurance | Enter the plan name for the member. |
| 6 | BIN #-Insurance | Enter the BIN number from the member ID Card. |
| 7 | Processor Control #-Insurance | Enter the PCN number from the member ID card. |
| 8 | CMS Part D Defined Qualified Facility | Enter a "Y" or "N" if the pharmacy is a CMS Part D Defined Qualified Facility. |
| 9 | Last-Member | Enter the member last name. |
| 10 | First-Member | Enter the member first name. |
| 11 | Person Code-Member | Enter the three digit person code. |
| 12 | D.O.B.-Member | Enter the member date of birth in MM-DD-CCYY format. |
| 13 | Gender-Member | Enter the member gender code. |
| 14 | Relationship-Member | Enter the relationship code between the member and cardholder. |
| 15 | Member Residence-member | Enter the member residence code. |
| 16 | DO NOT USE | Leave this field blank. |
| 17 | Service Provider ID-Pharmacy | Enter the pharmacy ID. |
| 18 | Qualifier-Pharmacy | Enter the service provider ID qualifier code. |
| 19 | Name-Pharmacy | Enter the name of the pharmacy. |
| 20 | Telephone #-Pharmacy | Enter the telephone number for the pharmacy. |
| 21 | Address-Pharmacy | Enter the address of the pharmacy. |
| 22 | City-Pharmacy | Enter the city of the pharmacy. |
| 23 | State-Pharmacy | Enter the State of the Pharmacy. |
| 24 | Zip-Pharmacy | Enter the zip code for the pharmacy. |
| 25 | Signature of Provider | The provider must sign this field. |
| 26 | Date | Enter the date in which the provider signed the paper claim. |
| 27 | ID-Prescriber | Enter the ID for the prescribing provider. |
| 28 | Qualifier-Prescriber | Enter the prescriber ID qualifier. |
| 29 | Last Name-Prescriber | Enter the prescriber's last name. |
| 30 | ID-Pharmacist | Enter the pharmacist's ID number. |
| 31 | Qualifier-Pharmacist | Enter the pharmacist's ID qualifier. |
| 32 | Prescription/Service Ref. #-Claim | Enter the Prescription or reference number. |
| 33 | Qual-Claim | Enter the prescription or service ID qualifier. |
| 34 | Fill #- Claim | Enter the fill number. |
| 35 | Date Written-Claim | Enter the date the prescription was written. |
| 36 | Date of Service-Claim | Enter the date of service. |
| 37 | Submission Clarification-Claim | Enter the submission clarification code. |
| 38 | Prescription Origin-Claim | Enter the prescription origin code. |
| 39 | Pharmacy Service Type-Claim | Enter the pharmacy service type code. |
| 40 | Special Packaging Indicator-Claim | Enter the special packaging indicator code. |
| 41 | Product/Service ID-Claim | Enter the product/service ID. |
| 42 | Qual-Claim | Enter the product/service ID qualifier. |
| 43 | Product Description-Claim | Enter the product description. |
| 44 | Quantity Dispensed-Claim | Enter the quantity dispensed. |
| 45 | Days Supply-Claim | Enter the days supply dispensed. |
| 46 | DAW Code- Claim | Enter the appropriate DAW code. |
| 47 | Prior Auth # Submitted-Claim | Enter the prior authorization number submitted. |
| 48 | PA Type-Claim | Enter the prior authorization type code. |
| 49 | Other Coverage-Claim | Enter the appropriate other coverage code, if applicable. |
| 50 | Delay Reason-Claim | Enter the appropriate delay reason code. |
| 51 | Level of Service-Claim | Enter the level of service. |
| 52 | Place of Service-Claim | Enter the place of service. |
| 53 | Quantity Prescribed-Claim | Enter the total quantity prescribed. |
| 54 | Diagnosis Code-Clinical | Enter the appropriate diagnosis code. |
| 55 | Qual-Clinical | Enter the diagnosis code qualifier. |
| 56 | DUR/PPS Codes- Reason-DUR | Enter the DUR/PPS reason for service code. |
| 57 | DUR/PPS Codes-Service-DUR | Enter the DUR/PPS service code. |
| 58 | DUR/PPS Codes-Result-DUR | Enter the DUR/PPS result of service code. |
| 59 | Level of Effort-DUR | Enter the level of effort-required when billing a compound. |
| 60 | Procedure Modifier-DUR | Enter the procedure modifier. |
| 61 | Other Payer ID-COB 1 | Enter the other payer ID when COB is present. |
| 62 | Qual-COB 1 | Enter the other payer ID qualifier. |
| 63 | Other Payer Date-COB 1 | Enter the date in which the other payer paid the claim. |
| 64 | Other Payer Rejects-COB 1 | Enter the other payer reject codes (maximum of 3). |
| 65 | Other Payer ID-COB 2 | Enter the other payer ID when COB is present. |
| 66 | Qual-COB 2 | Enter the other payer ID qualifier. |
| 67 | Other Payer Date-COB 2 | Enter the date in which the other payer paid the claim. |
| 68 | Other Payer Rejects-COB 2 | Enter the other payer reject codes (maximum of 3). |
| 69 | Dosage Form Description Code-Compound | Enter the dosage form description code. |
| 70 | Dispensing Unit Form Indicator-Compound | Enter the dispensing unit form indicator. |
| 71 | Route of Administration | Enter the SNOMED route of administration code. |
| 72 | Ingredient Component Count-Compound | Enter the ingredient component count code. |
| 73 | Product Name-Compound | Enter the product name (maximum of 25). |
| 74 | Product ID-Compound | Enter the product ID (maximum of 25). |
| 75 | Qual-Compound | Enter the product ID number qualifier (maximum of 25). |
| 76 | Ingredient QTY-Compound | Enter the ingredient quantity. |
| 77 | Ingredient Drug Cost-Compound | Enter the ingredient drug cost associated with the product ID. |
| 78 | Basis of Cost-Compound | Enter the basis of cost code. |
| 79 | Usual & Customary Charge-Pricing | Enter the usual and customary charge. |
| 80 | Basis of Cost Det.-Pricing | Enter the basis of cost determination. |
| 81 | Ingredient Cost Submitted Enter | Enter the submitted ingredient cost. |
| 82 | Dispensing Fee Submitted-Pricing | Enter the submitted dispensing fee. |
| 83 | Prof Service Fee Submitted-Pricing | Enter the submitted professional service fee. |
| 84 | Incentive Amount Submitted-Pricing | Enter the submitted incentive amount. |
| 85 | Other Amount Submitted-Pricing | Enter the submitted other amount. |
| 86 | Sales tax Submitted-Pricing | Enter the submitted sales tax. |
| 87 | Gross Amount Due (submitted)-Pricing | Enter the submitted gross amount due. |
| 88 | Member Paid Amount | Enter the amount paid by the member. |
| 89 | Other Payer Amount Paid #1-Pricing | Enter the other payer amount paid by the first other payer (if present). |
| 90 | Other Payer Amount Paid #2 | Enter the other payer amount paid by the second other payer (if present). |
| 91 | Other Payer Member Resp. Amount #1-Pricing | Enter the other payer member responsibility amount from the first other Payer (if present). |
| 92 | Payer Member Resp. Amount #2-Pricing | Enter the other payer member responsibility amount from the second other Payer (if present). |
| 93 | Net Amount Due-Pricing | Enter the net amount due. |
End of Billing a Paper Claim Chapter
Appendix A: Forms
The forms below and others are available on the Forms page of the Provider Information website:
- Drug Prior Authorization Form
- Individual Adjustment Request
- Link Request, Montana Access to Health Web Portal
- Prescription Claim Form UCF (Universal Claim Form Version 1.2-02/2013)
End of Appendix A: Forms Chapter
Definitions and Acronyms
End of Definitions and Acronyms Chapter
Search Options
This edition has three search options.
- Search the whole manual. Open the Complete Manual tab. From your keyboard press the Ctrl and F keys at the same time. A search box will appear. Type in a descriptive or key word (for example "Denials"). The search box will show all locations where denials are discussed in the manual.
- Search by Chapter. Open any Chapter tab (for example the "Billing Procedures" tab). From your keyboard press the Ctrl and F keys at the same time. A search box will appear. Type in a descriptive or key word (for example "Denials"). The search box will show where denials are discussed in just that chapter.
- Site Search. Search the manual as well as other documents related to a particular search term on the Site Specific Search page.